
Treasury Board of Canada Secretariat
www.tbs-sct.gc.ca
Common menu bar links
Breadcrumb Trail
ARCHIVED - Health Canada - Report
 This page has been archived.
This page has been archived.
Archived Content
Information identified as archived on the Web is for reference, research or recordkeeping purposes. It has not been altered or updated after the date of archiving. Web pages that are archived on the Web are not subject to the Government of Canada Web Standards. As per the Communications Policy of the Government of Canada, you can request alternate formats on the "Contact Us" page.
Minister's Message

The Departmental Performance Report for 2009-2010 summarizes Health Canada's accomplishments and its ongoing work on key health priorities for this period. The Department continues to implement strategies that focus attention on, and resources to, areas with the greatest potential benefits for Canadians. Health Canada is turning to new ideas, information, and approaches to guide its choices to achieve better immediate and long-term health outcomes.
For several years now, First Nations and Inuit health has been a key priority for our Department. While we can point with some pride to the improvements in the health outcomes of Aboriginal people in Canada, obvious gaps remain. Our Government recognized this, and provided needed financial support for First Nations and Inuit health services through Budget 2009. We also provided critical funding, through Canada's Economic Action Plan, to improve health facilities and nurses' residences in many First Nations and Inuit communities. We recognize the importance of longer-term change and, as a result, we continued working with First Nations and provincial government partners to achieve better integration of First Nations health services with provincial health systems.
Through collaboration with provincial and territorial governments and other partners, we are working towards our short-term goals while pursuing longer-term goals that will make Canada's health system more responsive to the needs of Canadians. For example, we worked to minimize the impact of supply shortages of medical isotopes and expedited the review of alternative isotope sources, continued investments to provide Canada's communities with the skilled health professionals they need, and we increased funding to the provinces and territories as they explored improvements in patient wait times. Canadians have seen changes, and they are also seeing results, some of which are making individual differences now and others that are setting the stage for more fundamental improvements in the years ahead.
Our Government's Food and Consumer Safety Action Plan, along with our environmental health activities, offer additional examples of our commitment to bring about changes that have immediate impacts and that lead to long-term benefits for Canadians. Health Canada is addressing the health needs of Canadians: whether by applying the Air Quality Health Index to Canadians in more communities; testing chemicals for health impacts; improving how health and consumer product safety concerns are reported and communicated; or implementing important tobacco regulations. At the same time, our work on new consumer product safety legislation and on modernizing important health and safety-related laws, demonstrates our Government's commitment to leading the change that will improve the health and safety of Canadians.
It is important to remember that this progress took place during the same year that Canadians witnessed the sudden emergence of H1N1 influenza. Health Canada worked with the Public Health Agency of Canada and other partners to implement the Canadian Pandemic Influenza Plan. We also worked closely with officials in other countries to pave the way for the accelerated testing and approval of new vaccines and the continuous improvement of response strategies and information that helped limit the impact of H1N1 on Canadians. While Health Canada had to adjust its plans, priorities, and resources to deal effectively with H1N1, we were still able to deliver on key commitments. We will continue to meet new challenges that arise and work to improve the health and wellbeing of Canadians-now and in the future.
The Honourable Leona Aglukkaq, P.C., M.P.
Minister of Health
Section I - Departmental Overview
Raison d'�tre
Responsibilities
Health Canada has many roles and responsibilities that help Canadians maintain and improve their health. First, as a regulator, Health Canada is responsible for the regulatory regimes governing the safety of products including food, pharmaceuticals, medical devices, natural health products, consumer products, chemicals, radiation emitting devices, cosmetics and pesticides. It also regulates tobacco products and controlled substances, public health on aircraft, ships and other passenger conveyances, and helps manage the health risks posed by environmental factors such as air, water, radiation and contaminants.
The Department is also a service provider. Improving the health of Aboriginal people is a shared responsibility among the federal, provincial, and territorial governments, and Aboriginal partners. Health Canada supports: basic primary care services in remote and isolated First Nations communities; home and community care in First Nations and Inuit communities; community-based health programs for First Nations and Inuit, focussing on children and youth, mental health and addictions, and chronic disease and injury prevention; and public health programs for First Nations, including communicable disease control. The Department also provides a limited range of medically-necessary health-related goods and services to eligible First Nations and Inuit that are not otherwise provided through other public programs or private insurance plans.
Health Canada is a catalyst for innovation, a funder, and an information provider in Canada 's health system. It works closely with provincial and territorial governments to develop national approaches on health system issues and promotes the pan-Canadian adoption of best practices. It administers the Canada Health Act, which embodies national principles to ensure a universal and equitable publicly-funded health care system. It provides policy support for the federal government's Canada Health Transfer to provinces and territories, and provides funding through grants and contributions to various organizations to help meet Health Canada's objectives. The Department draws on leading-edge science and policy research to generate and share knowledge and information to support decision-making by Canadians, development and implementation of regulations and standards, and health innovation.
Comprising over 30% of Health Canada's staff, regional operations represent the face of the Department to the people of Canada and support all of Health Canada's strategic outcomes. In 2009-2010 Health Canada 's regions continued to be a key strategic business partner by delivering services in the areas of First Nations and Inuit health - including H1N1 vaccinations on-reserve; occupational health and safety; inspection and surveillance; health products and food; and, prevention and treatment of illicit drug use and abuse.
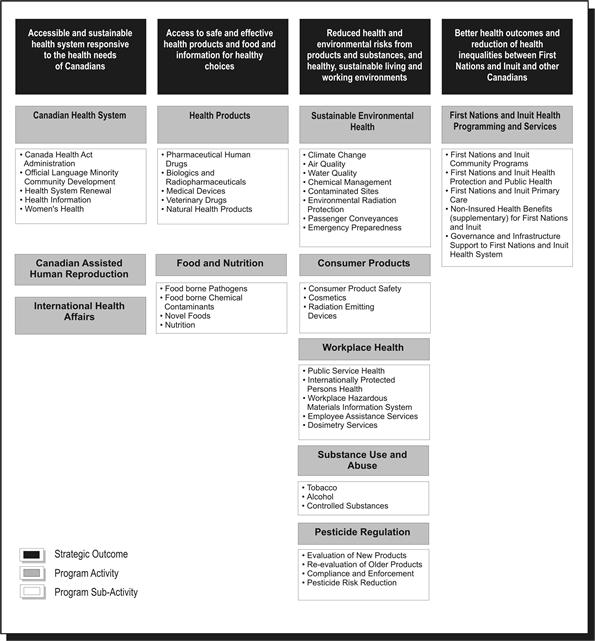
Strategic Outcome(s) and Program Activity Architecture (PAA)
In order to pursue its mandate most effectively and allocate resources appropriately, Health Canada has identified four strategic outcomes, each of which is supported by a framework of program activities and sub-activities.
Planning Summary
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 3,587.0 | 3,813.3 | 3,748.9 |
Health Canada's financial resources directly impacted the ability of the Department to achieve its strategic outcomes and deliver on its program activities. The following sections will highlight Health Canada's performance and demonstrate linkages between resources and results.
At the outset of the 2009-10 fiscal year, Health Canada's planned spending was $3,587 million. Through Main Estimates and Supplementary Estimates, the department was allocated total authorities of $3,813.3 million. Actual spending for Health Canada was $3,748.9 million.
| Planned | Actual | Difference |
|---|---|---|
| 9,914 | 9,756 | 158 |
The human resources table above provides a summary of the total planned human resources and actual human resources for Health Canada for fiscal year 2009-10.
Performance Summary Table
| Performance Indicators | Targets | 2009-10 Performance |
|---|---|---|
|
Percentage of Canadians reporting timely access |
Increased number of Canadians reporting timely access (baseline is 80% of Canadians reporting timely access taken from the Health Services Access Survey, published in 2006) |
In 2009(**) 84.9% of Canadians, aged 12 and older, reported having a regular medical doctor, compared to 84.4% in 2008 and 84.9% in 2007. (*) The most recent figures from Statistics Canada show that most Canadians requiring routine or ongoing health services, health information or advice, and immediate care for a minor health problem do not report difficulties obtaining them. The percentage of Canadians self-reporting timely access to routine or ongoing health services was 82.8% in 2007 compared to 83.6% reported in 2003 and 2005.(*) In the 2007 survey, the percentage of Canadians self-reporting timely access to immediate care for a minor health problem was 74.7% compared to 79.3% in 2005 and 76.2 in 2003. The percentage of Canadians self-reporting timely access to health information or advice was 83.2% in 2007, compared with 85% in 2005 and 84.2% in 2003. |
| Percentage of Canadians satisfied with quality of primary, acute, chronic and continuing health care service | Increased number of Canadians satisfied with overall quality of health services (baseline is 85% of Canadians taken from Canadian Community Health Survey published in 2006) | In 2007, 85.2% of Canadians reported being "very satisfied" or "somewhat satisfied" with the way overall health care services were provided. Also, 89.8% of Canadians who received care from a physician reported being "very satisfied" or "somewhat satisfied" with the way physician care was provided. (*) |
| Increased sustainability of the health system through the development of new initiatives (long-term funding commitments, primary health care reform, use of science and technology) |
Increased number of initiatives that improve sustainability in the health system |
Initiatives relating to improved sustainability of the health care system included: |
Performance Data is from either:
(*) Healthy Canadians: A federal report on comparable health indicators, 2008 or
(**) Statistics Canada. Cansim Table 105-0501 - Health indicator profile, annual estimates, by age group and sex, Canada, provinces, territories, health regions (2007 boundaries) and peer groups, occasional,
CANSIM (database).
| Program Activity | 2008-09 Actual Spending |
2009-10 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Canadian Health System | 533.9 | 293.3 | 305.1 | 377.7 | 369.4 | Healthy Canadians |
| Canadian Assisted Human Reproduction | 3.9 | 1.5 | 1.5 | 2.6 | 2.6 | |
| International Health Affairs | 25.6 | 23.0 | 23.0 | 21.5 | 19.3 | |
| Total for SO 1 | 563.4 | 317.8 | 329.6 | 401.8 | 391.3 | |
| Performance Indicators | Targets | 2009-10 Performance |
|---|---|---|
| Increased rate of adherence to/compliance by industry with the Food and Drugs Act and its regulations, standards and guidelines (level of adherence/compliance of registered establishment by sector (e.g., meat, dairy, fish and seafood, processed food, shellfish and egg). |
Human drugs: 98% compliance; |
Human drugs: 96.0% compliance with the Food and Drugs Act Natural Health Products: baseline still to be established, as required. Medical Devices: An updated inspection program for medical devices, to be implemented in fall 2010, is expected to provide a measure of industry compliance with the Food and Drugs Act and regulations, standards and guidelines |
| Increased public confidence in available information related to health products, food and nutrition | 50% of Canadians are confident in the safety of the Canadian food supply (baseline data in 2006: 42%) |
A February 2010 survey conducted by Ekos regarding Canadians' knowledge and behaviour related to food safety indicates that 63% of Canadians are confident in Canada's food safety system. Over three in four say they feel they have enough information about food safety and how to protect themselves and their families from food-borne illnesses. |
| Program Activity | 2008-09 Actual Spending |
2009-10 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Health Products | 255.9 | 146.1 | 146.4 | 191.8 | 191.2 | Healthy Canadians |
| Food and Nutrition | 61.7 | 60.9 | 60.9 | 53.5 | 53.5 | |
| Total for SO 2 | 317.6 | 207.0 | 207.3 | 245.3 | 232.7 | |
| Performance Indicators | Targets | 2009-10 Performance |
|---|---|---|
| Number of incidents of deaths, exposures, illness, injury and adverse reactions. | Baseline information to be established in the next one to three years for defined populations. |
Until a new legislative framework for consumer products is in effect which imposes mandatory reporting, the number of consumer complaints is being used as an interim proxy performance indicator. Product Safety Complaints/Incidents showed an increasing trend: 2006-07, 567 complaints; 2007-2008, 672 complaints; 2008-2009, 944 complaints; 2009-2010, 1102 complaints. The increase in complaints by consumers is an indication of increased consumer awareness of risks associated with consumer products. Of the 1102 complaints received in 2009-2010, Health Canada met its service targets, responding to 100% of complainants and met its service standard following-up with 100% of companies. Depending on the severity of the incident reported, actions included product inspection with follow-up and enforcement actions, including recall or public advisory, as appropriate, and follow-up with the companies in question to ensure appropriate actions have been completed. |
| Proportion of regulatory actions addressed within service standards/targets. | To be set after baseline is established in 2011. |
Risk management actions were imposed on 100% of substances for which a significant risk was identified (20/20). Risk Management Instruments were developed for identified substances within expected timelines. 100% of human health risk assessments related to high priority federal contaminated sites were addressed within planned timelines. Screening assessment reports for Challenge and non-Challenge substances under the Chemicals Management Plan, were completed and published in the Canada Gazette Part I according to departmental timelines. |
| Percentage of inspected or verified registrants / firms / users compliant / non-compliant. | Baseline information to be established in the next one to three years for defined populations. | 84.3% of tobacco retailers are in compliance with regulations restricting underage youth from purchasing tobacco products, marking a significant increase from 69.8% in 2000. |
| Program Activity | 2008-09 Actual Spending |
2009-10 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Sustainable Environmental Health | 165.5 | 152.9 | 153.3 | 135.2 | 130.5 | Healthy Canadians |
| Consumer Products | 29.4 | 25.6 | 25.6 | 27.9 | 27.3 | |
| Workplace Health | 51.5 | 23.0 | 23.0 | 31.2 | 35.7 | |
| Substance Use and Abuse | 118.4 | 138.6 | 138.7 | 113.7 | 104.6 | |
| Pesticide Regulation | 64.5 | 45.1 | 45.1 | 54.1 | 49.5 | |
| Total for SO 3 | 429.3 | 385.2 | 385.7 | 362.1 | 347.6 | |
| Performance Indicators* | Targets | 2009-10 Performance |
|---|---|---|
| Life expectancy (at birth, by gender, on and off reserve), comparison of First Nations and Inuit with other Canadians | The Department will continue to work with others toward reducing these inequalities | Life Expectancy - The most recent data (2001) estimated life expectancy for First Nations at 70.4 years for males and 75.5 years for females; and for Inuit at 64.4 years for males and 69.8 years for females (Canadian average: males 77 years, females 82 years). |
| Birth weight (comparison of First Nations and Inuit with other Canadians) | Statistics from 2002-2003 indicate that 5.5% of First Nations on-reserve births are classified as low birth weight compared with 6.0% in Canada overall. The high birth weight rate for First Nations on-reserve is 21% approximately double the Canadian rate of 13%. Comparatively, the low birth rate among Inuit-inhabited areas (1999-2000) is 6.7% and the high birth rate is 13.1%. Health Canada is working in maternal and prenatal health to improve these outcomes. | |
| Mortality rates | Overall mortality for First Nations (2000) is 1.4x higher than for the Canadian population (1999) (based on age-standardized rates for regions with available data) | |
| Infant mortality rates | Reliable infant mortality data is currently not available. | |
|
Rates of conditions by type - e.g., diabetes, suicide, tuberculosis |
Diabetes Rates - 19.7% for First Nations on-reserve (most recent data 2002/2003) - 3.8 times higher than the Canadian average 3% in Inuit regions (most recent data 2005/2006) - below the Canadian average (5.1%) Suicide Rates - The rate of First Nations youth suicide (10 to 19 years) was 4.3 times greater than the Canadian average in 2000. The rate for Inuit regions (1999-2003) is 11.6 times higher than the Canadian average. Incidence of Tuberculosis - Registered Indians 5.9 times higher and Inuit regions 17.9 times higher than the general Canadian population (4.7 cases per 100,000 population |
*Note: Health Canada continues to work with its federal (e.g. Statistics Canada, Indian and Northern Affairs Canada) provincial and territorial partners as well as with First Nations and Inuit to improve the quality and accessibility of performance indicator data. Many indicators (e.g. life expectancy, mortality) only show changes over the very long-term.
| Program Activity | 2008-09 Actual Spending |
2009-10 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| First Nations and Inuit Health Programming and Services | 2,357.8 | 2,156.1 | 2,361.3 | 2,414.3 | 2,392.8 | Healthy Canadians |
| Total for SO 4 | 2,357.8 | 2,156.1 | 2,361.3 | 2,414.3 | 2,392.8 | |
| Program Activity | 2008-09 Actual Spending |
2009-10 | Alignment to Government of Canada Outcomes |
|||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Internal Services* | 0.0 | 302.6 | 303.1 | 389.8 | 384.5 | |
| Total for Internal Services | 0.0 | 302.6 | 303.1 | 389.8 | 384.5 | |
*Note: Commencing in the 2009-2010 Estimates cycle, the resources for Program Activity Internal Services is displayed separately from other program activities; they are no longer distributed among remaining program activities, as was the case in previous Main Estimates. This has affected the comparability of spending and FTE information by Program Activity between fiscal years.
Contribution of Priorities to Strategic Outcome(s)
Health Canada applied the performance status rating as defined by Treasury Board of Canada Secretariat in their Guide to the Preparation of Part III of the 2010-11 Estimates.
- Exceeded - More than 100 per cent of the expected level of performance (as evidenced by the indicator and target or planned activities and outputs) for the expected result or priority identified in the corresponding RPP was achieved during the fiscal year.
- Met All - 100 per cent of the expected level of performance was achieved during the fiscal year.
- Mostly Met - 80 to 99 per cent of the expected level of performance was achieved during the fiscal year.
- Somewhat Met - 60 to 79 per cent of the expected level of performance was achieved during the fiscal year.
- Not Met - Less than 60 per cent of the expected level of performance was achieved during the fiscal year.
| Operational Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
I. Modernized safety framework: a) Continue implementation of Canada's Food and Consumer Safety Action Plan |
Ongoing |
Performance Status: mostly met a) The Department continued to work towards modernizing its legislative framework for parliamentary consideration, and has made strides to move regulatory activities forward. Continued regulatory oversight and guidance to industry was provided for health products by initiating pre-submission meetings intended to increase awareness and compliance with regulatory requirements. There was an increase in post-market surveillance activities and collaboration with stakeholders as well as an increase in voluntary adverse reaction reporting and an increase in post-market surveillance plans from industry. Health Canada has improved targeted consumer risk communication to increase public understanding of food safety risks and alert and safety systems. Health Canada continues to address areas of high risk and concern through ongoing targeted inspections, surveillance and compliance promotion under the existing legislation, and outreach to Canadians on the potential dangers associated with some consumer products. |
2 and 3 |
| b) Strengthen measures on tobacco control with respect to children and youth | Ongoing |
Performance Status: met all b) Bill C-32, Cracking Down on Tobacco Marketing Aimed at Youth Act, received Royal Assent in October 2009, and is expected to contribute to the reduced use of tobacco products by Canadian youth. |
2 and 3 |
| Operational Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
II. Strengthen First Nations and Inuit health programming: a) Stabilize First Nations and Inuit health system to support harmonization with provincial programs |
Ongoing |
Performance Status: met all a) Health Canada maintained its standards of care for First Nations and Inuit health programs and services. Canada's Economic Action Plan provided $67.4 million in 2009-2010 for the construction and renovation of health services infrastructure for First Nations, including health centres and nurses' residences. An additional investment of $134.5 million supported the Non-Insured Health Benefits program and the delivery of primary care nursing services in remote and isolated First Nations communities. The Aboriginal Health Transition Fund (AHTF) has improved integration of federally and provincially funded health services and adaptation of provincial and territorial health programs to meet the unique needs of First Nations and Inuit. This is occurring through the development of multi-partner joint service protocols, referral/discharge and information systems, collaborative committees, and governance structures and/or processes. |
4 |
| b) Continue integration of federal/provincial/ territorial First Nations health programs and services through tripartite agreements | Ongoing |
Performance Status: met all b) Health Canada, the British Columbia government and the British Columbia First Nations Leadership Council continue to work toward implementation of the commitments made in the 2007 Tripartite First Nations Health Plan. Discussions among partners regarding a 10-year Saskatchewan Health and Wellness Plan are ongoing. |
4 |
| Operational Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
III. Health system innovation: Continue to work with the provincial/territorial governments on health human resources and other matters of national interest through focussed and innovative means |
Ongoing |
Performance Status: mostly met Working in collaboration with provincial and territorial governments, Health Canada supported the development and promotion of innovative ideas that can result in improved access, effectiveness and efficiency for the Canadian health care system. $20 million annually has been invested in the Pan-Canadian Health Human Resource Strategy to ensure the availability of appropriate, skilled, competent health professionals. Initiatives also include strategies to facilitate the integration of internationally-educated health professionals into Canada's health system and for demonstration projects designed to improve retention and recruitment of nurses. The Department is accelerating the implementation of Health Information Systems, via Canada Health Infoway, to support the continued implementation of electronic health records and other electronic health technologies (e.g. telehealth and public health surveillance). Health Canada is also providing advice and active support to the Canadian Institutes of Health Research led Drug Safety and Effectiveness Network The Department supported all provincial and territorial governments in progress toward establishing Patient Wait Times Guarantees (PWTGs) in at least one of the priority clinical areas with funding through the three-year PWTG Trust and the PWTG Pilot Project Fund, both of which ended March 31, 2010. PWTG pilot projects were completed in eight jurisdictions. By April 2010, nine of ten provinces had established guarantees with the remaining province and three territories indicating they would do so later in 2010. A March 2010 Canadian Institute for Health Information study shows that most patients are now receiving care within recommended wait times for priority procedures: hip fracture repairs or replacements, cataract surgery, and cancer radiation therapy. |
1, 2 and 3 |
| Management Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
IV. Increase quality and coherence of strategic policy: a) Talent Management Framework |
Ongoing |
Performance Status: mostly met a) The Health Canada Talent Management Strategy, an initiative for maximizing the Department's investment in human resources at all levels and all areas of expertise, proceeded on schedule, although fiscal pressures to meet costs related to H1N1 and required budget reductions led to reallocations that delayed some elements of the strategy. |
1, 2, 3 and 4 |
| b) Ensure all policy is evidence-based by better integrating science/research in the policy development process | Ongoing |
Performance Status: met all b) A Health Canada Science Plan was developed to strengthen links between science and decision-making in the Department. Based on extensive consultations, department-wide science needs have been identified to establish science priorities, as well as priorities for policy work and related evidence gathering and analysis over the longer term. Centres of Expertise were established to provide guidance within the Department, for: nanotechnology, science and technology foresight, bioethics, and risk assessment. A Science Excellence Framework was also developed. |
1, 2, 3 and 4 |
| Management Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
V. Enhance corporate processes for increased accountability: a) Strengthen integrated planning b) Improve performance measurement and indicators |
Ongoing |
Performance Status: met all a) Through continual process and technology improvements, departmental operational planning has begun integrating business plans with financial, HR, IT, investment planning and facilities management. Performance Status: met all b) A review was conducted on Health Canada's Program Activity Architecture and work began to update this structure and to develop a Performance Measurement Framework for implementation with the 2011/2012 planning cycle. The revised PAA will include updated performance indicators that will improve the objective basis for evaluating the performance of programs. |
This management priority is part of the Internal Services Program Activity which contributes to all strategic outcomes |
|
c) Enhanced Financial Management Control Framework |
Ongoing |
Performance Status: met all c) The Department incorporated a series of measures to equip its staff to manage financial risks, by: raising awareness; providing appropriate knowledge and tools; training and development in financial management; and, by documenting main business processes and key risk and control points to support the management and oversight of its control systems. In preparing for auditable financial statements, the Department completed the documentation of key business processes and related internal controls over financial reporting. |
This management priority is part of the Internal Services Program Activity which contributes to all strategic outcomes |
| Management Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
VI. Increase transparency and innovative engagement with Canadians a) Strengthen departmental frameworks and policies for engaging Canadians |
Ongoing |
Performance Status: met all a) Work continued toward a Departmental Action Plan to support better integration of fundamental public involvement principles on openness/transparency/accountability in departmental decision making. An implementation plan to ensure the consistent understanding and application of a departmental Consumer Information Strategy was developed for implementation in the new fiscal year. New software tools to track general consumer inquiries phone calls and e-mails about regulated products were put in place to allow us to measure call volume and improvements in response time. Health Canada used social media tools that provide access to information for consumers, health professionals and industry when, where and how they want it. |
1, 2 and 3 |
| b) Better communication with Canadians and our stakeholders, and improve public's access to health and safety information | Ongoing |
Performance Status: met all b) Health Canada made strides in making food, health and consumer product information more accessible, credible and more consumer friendly, for example:
|
1, 2 and 3 |
Risk Analysis
Over the last fiscal year, a number of risks were faced by the Department and needed to be managed in order to achieve the Department's mandate and strategic objectives. Also, there were three major external incidents that influenced the year's events for Health Canada. The first was the pace of progress on the Food and Consumer Safety Action Plan. In particular, the legislative process surrounding Bill C-6, the proposed Canada Consumer Product Safety Act, did not receive Royal Assent. Without the Royal Assent necessary for the Department to proceed on key changes, it was not possible to deliver all the expected results for the year.
The second event was the emergence of H1N1 influenza in April 2009. Health Canada management shifted much of its focus, and substantial resources, to the work necessary to understand and address H1N1 in Canada and to work with partners on international aspects of the H1N1 response. Health Canada reallocated resources from lower-priority commitments to ensure that a new vaccine would be available for all Canadians and emergency interventions could be improved. Joint measures were conducted in partnership with the Public Health Agency of Canada to ensure a coordinated response to national health risks and protect the well-being of Canadians.
The Department took similar action to support the Government in addressing the impact on access to medical isotopes after the shutdown of the Chalk River nuclear reactor. Alternative sources of isotopes around the world were identified and used by provincial and territories health establishments to secure isotope supplies, while the Department also identified the value of planning for similar medical situations in ways that take into account the complex interplay of medical, social and business interests.
Beyond that, other elements of the risk analysis set out in the RPP were managed during the year. Health Canada applied the lessons learned from the 2008 listeriosis outbreak. This led to actions such as a revision of roles between organizations and evaluation of options to increase laboratory capacity and access. In collaboration with the Canadian Food Inspection Agency (CFIA) and the Public Health Agency of Canada (PHAC), public health officials and provincial and territorial Ministries of Health, Health Canada revised its policy on Listeria monocytogenes in ready-to-eat foods that would have impacts on the Canadian Food Inspection Agency, provincial/territorial governments and food industry as they identify steps to reduce the risk of Listeria contamination in these foods. Health Canada briefed the medical community, public health officials, the food industry and the public on matters related to listeriosis, and participated in public awareness campaigns about safe food practices.
Health Canada recognized the risks associated with the growing expectation and need for information from the public in a context where the information is globalized and made available 24 hours a day, and where science and technology rapidly evolve. For example, the Department supported the development and dissemination of health knowledge and information through the funding for the Canadian Institute for Health Information; by ensuring a consistent approach to communicating risks and benefits of regulated products; and by dedicated resources to better explain health risks to Canadians.
In a context of declining fiscal flexibility for the Government of Canada, the Department acknowledged that financial integrity of key programs could be at risk, considering for example challenges from increasing costs of its regulatory activities, outdated user fee regimes, and the ongoing need to support First Nations and Inuit health services. To ensure the sustainability of key programs: Health Canada reallocated funds to align with priorities; conducted monthly financial reviews to manage resources effectively; moved to secure increased cost-recovery revenues through new user fees proposals; and obtained additional funding for First Nations and Inuit health programs and benefits.
Health Canada addressed risks associated with managing horizontal initiatives such as the Chemicals Management Plan, Clean Air Agenda, and Food and Consumer Safety Action Plan. In an effort to increase engagement with external partners, Health Canada built on and clarified existing roles, responsibilities and accountabilities in order to enhance collaboration and achieve outcomes. Lessons in optimizing horizontal external relationships will be important as the Department moves forward in its ongoing effort to support collaboration among federal, provincial and Aboriginal partners. These collaborative efforts support the improvement of health services for First Nations through enhanced integration and alignment of federal and provincial health systems as well as increased First Nations and Inuit capacity to design, deliver and manage their own health programs.
The Department also addressed risks associated with its internal management. Committed to develop policy based on cutting-edge science, the Department addressed associated risks through initiatives such as creation of a Science and Policy Integration Unit, a new Science and Policy Round Table and the Health Canada Science Forum. Health Canada also implemented initiatives to attract and retain key talent in the face of a competitive labour market and human resource challenges such as an aging work force, a high rate of staff eligible for retirement, the need to staff positions in remote locations and the need to respect official language commitments. The Department also continued to implement a reorganization that has addressed regional decision-making and accountability challenges.
Expenditure Profile
For the 2009-10 fiscal year, Health Canada spent $3,748.9 million to meet the expected results of its program activities and contribute to its strategic outcomes.
The figure below illustrates Health Canada's spending trend from 2007-2008 to 2009-2010.
Spending Trend
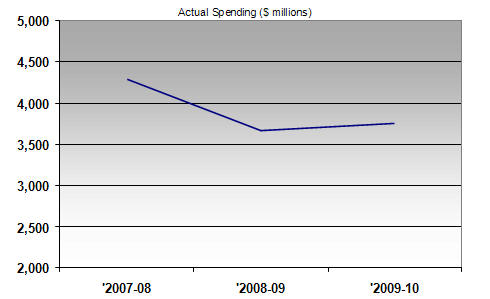
For the 2007-2008 to 2009-2010 periods, the total spending includes all Parliamentary appropriation sources: Main Estimates, Supplementary Estimates, Treasury Board collective bargaining, operating budget carry forward, and other special adjustments.
In 2007-08, actual spending was particularly high due to the $1 billion compensation payments to individuals infected with the Hepatitis C virus through the Canadian blood supply before 1986 and after 1990.
The table below offers a comparison of the Main Estimates, planned spending, total authorities and actual spending for the most recently completed fiscal year, as well as the historical actual spending figures for the previous year.
| Program activities | 2008-2009 Actual Spending |
2009-2010 Main Estimates |
2009-2010 Planned Spending |
2009-2010 Total Authorities |
2009-2010 Actual Spending |
|---|---|---|---|---|---|
|
Canadian Health System |
533.9 | 293.3 | 305.1 | 377.7 | 369.4 |
|
Canadian Assisted Human Reproduction |
3.9 | 1.5 | 1.5 | 2.6 | 2.6 |
|
International Health Affairs |
25.6 | 23.0 | 23.0 | 21.5 | 19.3 |
|
Health Products |
255.9 | 146.1 | 146.4 | 191.8 | 191.2 |
|
Food and Nutrition |
61.7 |
60.9 | 60.9 | 53.5 | 41.5 |
|
Sustainable Environmental Health |
165.5 |
152.9 | 153.3 | 135.2 | 130.5 |
|
Consumer Products |
29.4 | 25.6 | 25.6 | 27.9 | 27.3 |
|
Workplace Health |
51.5 | 23.0 | 23.0 | 31.2 | 35.7 |
|
Substance Use and Abuse |
118.4 | 138.6 | 138.7 | 113.7 | 104.6 |
|
Pesticide Regulation |
64.5 | 45.1 | 45.1 | 54.1 | 49.5 |
|
First Nations and Inuit Health |
2,357.8 | 2,156.1 | 2,361.3 | 2,414.3 | 2,392.8 |
|
Internal Services |
0.0 | 302.6 | 303.1 | 389.8 | 384.5 |
| Total Department |
3,668.1 |
3,368.7 |
3,587.0 |
3,813.3 |
3,748.9 |
Note: Commencing in the 2009-10 Estimates cycle, the resources for Program Activity: Internal Service is displayed separately from other program activities; they are no longer distributed among the remaining program activities, as was the case in previous Main Estimates. This has affected the comparability of spending and FTE information by Program Activity between fiscal years.
The $218.3 million increase from Main Estimates to Planned Spending is due to anticipated funding from the Government's Economic Action Plan to stabilize the Non-Insured Health Benefits program and primary care services and a direct investment for construction and renovation of infrastructure for First Nations and Inuit health services, as well as anticipated additional funding relating to the Official Languages Health Contribution Program.
The $226.3 million increase from Planned Spending to Total Authorities is due to new program initiatives received through Supplementary Estimates, including funding for addressing the first and second wave of the H1N1 flu virus outbreak, for providing mental health and emotional support services and the administration and research required to support the federal government's obligations under the Indian Residential Schools Settlement Agreement, and for addressing the submission review backlog in the Natural Health Products Program.
The $64.4 million difference between Total Authorities and Actual Spending was mainly the result of lapses in TB special purpose allotments for H1N1, the Indian Residential Schools Settlement Agreement, and Health Council, as well as in the TB frozen allotment for the National Anti-Drug Strategy (Mandatory Minimum Penalties).
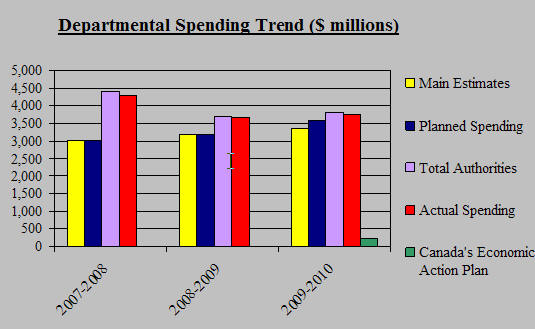
Canada's Economic Action Plan (CEAP)
Health Canada was allocated $211.9 M in 2009-2010, for initiatives under Canada's Economic Action Plan (CEAP). They are:
- $0.3 M for a one-year extension for Canadian Environmental Sustainability Indicators;
- $134.5 M to strengthen the Non-Insured Health Benefits program and enhance support for primary care services for First Nations and Inuit;
- $67.4 M for infrastructure investments through the Health Facilities and Capital Program for First Nations and Inuit;
- $9.0 M for investments in the maintenance and modernization of Health Canada laboratories;
- $0.7 M for maintenance or upgrading of existing Arctic research facilities (facilities transferred from INAC to HC in 2009-2010).
In addition, $500 M announced in the 2009 Budget and confirmed in Budget 2010, will be provided to Canada Health Infoway, which will be governed by the terms and conditions of a new agreement.
Departamental Spending Trend
($ millions)
Voted and Statutory Items
The table below illustrates the way in which Parliament approved Health Canada's resources in 2008-09 and 2009-10 and shows, for 2009-10, changes in resource levels from planning to Main Estimates to final authorities, as well as the actual spending at year-end.
| Vote | 2008-2009 Actual Spending |
2009-10 Main Estimates |
2009-10 Planed Spending |
2009-10 Total Authorities |
2009-10 Actual Spending |
|---|---|---|---|---|---|
| Health Canada | |||||
| (1) Operating expenditures |
1,884.7 |
1,788.4 |
1,896.2 |
2,016.1 |
1,967.7 |
| (5) Capital expenditures |
40.9 |
40.8 | 41.6 | 53.5 | 47.0 |
| (10) Grants and contributions |
1,389.6 |
1,422.7 |
1,529.2 |
1,528.2 |
1,519.2 |
| (S) Minister of Health - Salary and motor car allowance | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 |
| (S) Spending of proceeds from the disposal of surplus Crown Assets | 0.1 | 0.0 | 0.0 | 0.9 | 0.4 |
| (S) Refunds from Previous Years Revenue | 0.2 | 0.0 | 0.0 | 0.9 | 0.9 |
| (S) Canada Health Infoway Inc | 123.0 | 0.0 | 0.0 | 64.9 | 64.9 |
| (S) Transfer payments to Mental Health Commission of Canada | 110.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| (S) Contributions to employee benefit plans |
119.5 |
116.7 |
119.9 |
139.8 |
139.8 |
| (S) Payments in connection with the Patent Act (Patented Medicines) | 0.0 | 0.0 | 0.0 | 9.3 | 9.3 |
| Total Department |
3,668.1 |
3,368.7 |
3,587.0 |
3,813.3 |
3,748.9 |
(S) Denotes statutory items which do not require an appropriation act