ARCHIVED - Health Canada - Report
 This page has been archived.
This page has been archived.
Archived Content
Information identified as archived on the Web is for reference, research or recordkeeping purposes. It has not been altered or updated after the date of archiving. Web pages that are archived on the Web are not subject to the Government of Canada Web Standards. As per the Communications Policy of the Government of Canada, you can request alternate formats on the "Contact Us" page.
2009-10
Departmental Performance Report
Health Canada
The original version was signed by
The Honourable Leona Aglukkaq P.C., M.P.
Minister of Health
Table of Contents
Section I: Departmental Overview
- Raison d'�tre
- Responsibilities
- Strategic Outcome(s) and Program Activity Architecture (PAA)
- 2009-2010 Financial Resources
- 2009-2010 Human Resources (FTEs)
- Contribution of Priorities to Strategic Outcomes
- Risk Analysis
- Expenditure Profile
- Canada's Economic Action Plan
- Voted and Statutory Items
Section II: Analysis of Program Activities by Strategic Outcome(s)
- Strategic Outcome 1
- Strategic Outcome 2
- Strategic Outcome 3
- Strategic Outcome 4
- Program Activity: Internal Services
Section III: Supplementary Information
Minister's Message

The Departmental Performance Report for 2009-2010 summarizes Health Canada's accomplishments and its ongoing work on key health priorities for this period. The Department continues to implement strategies that focus attention on, and resources to, areas with the greatest potential benefits for Canadians. Health Canada is turning to new ideas, information, and approaches to guide its choices to achieve better immediate and long-term health outcomes.
For several years now, First Nations and Inuit health has been a key priority for our Department. While we can point with some pride to the improvements in the health outcomes of Aboriginal people in Canada, obvious gaps remain. Our Government recognized this, and provided needed financial support for First Nations and Inuit health services through Budget 2009. We also provided critical funding, through Canada's Economic Action Plan, to improve health facilities and nurses' residences in many First Nations and Inuit communities. We recognize the importance of longer-term change and, as a result, we continued working with First Nations and provincial government partners to achieve better integration of First Nations health services with provincial health systems.
Through collaboration with provincial and territorial governments and other partners, we are working towards our short-term goals while pursuing longer-term goals that will make Canada's health system more responsive to the needs of Canadians. For example, we worked to minimize the impact of supply shortages of medical isotopes and expedited the review of alternative isotope sources, continued investments to provide Canada's communities with the skilled health professionals they need, and we increased funding to the provinces and territories as they explored improvements in patient wait times. Canadians have seen changes, and they are also seeing results, some of which are making individual differences now and others that are setting the stage for more fundamental improvements in the years ahead.
Our Government's Food and Consumer Safety Action Plan, along with our environmental health activities, offer additional examples of our commitment to bring about changes that have immediate impacts and that lead to long-term benefits for Canadians. Health Canada is addressing the health needs of Canadians: whether by applying the Air Quality Health Index to Canadians in more communities; testing chemicals for health impacts; improving how health and consumer product safety concerns are reported and communicated; or implementing important tobacco regulations. At the same time, our work on new consumer product safety legislation and on modernizing important health and safety-related laws, demonstrates our Government's commitment to leading the change that will improve the health and safety of Canadians.
It is important to remember that this progress took place during the same year that Canadians witnessed the sudden emergence of H1N1 influenza. Health Canada worked with the Public Health Agency of Canada and other partners to implement the Canadian Pandemic Influenza Plan. We also worked closely with officials in other countries to pave the way for the accelerated testing and approval of new vaccines and the continuous improvement of response strategies and information that helped limit the impact of H1N1 on Canadians. While Health Canada had to adjust its plans, priorities, and resources to deal effectively with H1N1, we were still able to deliver on key commitments. We will continue to meet new challenges that arise and work to improve the health and wellbeing of Canadians-now and in the future.
The Honourable Leona Aglukkaq, P.C., M.P.
Minister of Health
Section I - Departmental Overview
Raison d'�tre
Responsibilities
Health Canada has many roles and responsibilities that help Canadians maintain and improve their health. First, as a regulator, Health Canada is responsible for the regulatory regimes governing the safety of products including food, pharmaceuticals, medical devices, natural health products, consumer products, chemicals, radiation emitting devices, cosmetics and pesticides. It also regulates tobacco products and controlled substances, public health on aircraft, ships and other passenger conveyances, and helps manage the health risks posed by environmental factors such as air, water, radiation and contaminants.
The Department is also a service provider. Improving the health of Aboriginal people is a shared responsibility among the federal, provincial, and territorial governments, and Aboriginal partners. Health Canada supports: basic primary care services in remote and isolated First Nations communities; home and community care in First Nations and Inuit communities; community-based health programs for First Nations and Inuit, focussing on children and youth, mental health and addictions, and chronic disease and injury prevention; and public health programs for First Nations, including communicable disease control. The Department also provides a limited range of medically-necessary health-related goods and services to eligible First Nations and Inuit that are not otherwise provided through other public programs or private insurance plans.
Health Canada is a catalyst for innovation, a funder, and an information provider in Canada 's health system. It works closely with provincial and territorial governments to develop national approaches on health system issues and promotes the pan-Canadian adoption of best practices. It administers the Canada Health Act, which embodies national principles to ensure a universal and equitable publicly-funded health care system. It provides policy support for the federal government's Canada Health Transfer to provinces and territories, and provides funding through grants and contributions to various organizations to help meet Health Canada's objectives. The Department draws on leading-edge science and policy research to generate and share knowledge and information to support decision-making by Canadians, development and implementation of regulations and standards, and health innovation.
Comprising over 30% of Health Canada's staff, regional operations represent the face of the Department to the people of Canada and support all of Health Canada's strategic outcomes. In 2009-2010 Health Canada 's regions continued to be a key strategic business partner by delivering services in the areas of First Nations and Inuit health - including H1N1 vaccinations on-reserve; occupational health and safety; inspection and surveillance; health products and food; and, prevention and treatment of illicit drug use and abuse.
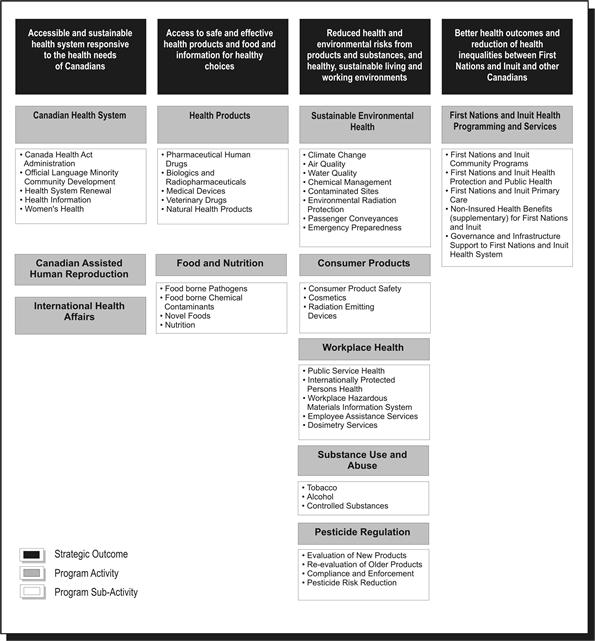
Strategic Outcome(s) and Program Activity Architecture (PAA)
In order to pursue its mandate most effectively and allocate resources appropriately, Health Canada has identified four strategic outcomes, each of which is supported by a framework of program activities and sub-activities.
Planning Summary
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 3,587.0 | 3,813.3 | 3,748.9 |
Health Canada's financial resources directly impacted the ability of the Department to achieve its strategic outcomes and deliver on its program activities. The following sections will highlight Health Canada's performance and demonstrate linkages between resources and results.
At the outset of the 2009-10 fiscal year, Health Canada's planned spending was $3,587 million. Through Main Estimates and Supplementary Estimates, the department was allocated total authorities of $3,813.3 million. Actual spending for Health Canada was $3,748.9 million.
| Planned | Actual | Difference |
|---|---|---|
| 9,914 | 9,756 | 158 |
The human resources table above provides a summary of the total planned human resources and actual human resources for Health Canada for fiscal year 2009-10.
Performance Summary Table
| Performance Indicators | Targets | 2009-10 Performance |
|---|---|---|
|
Percentage of Canadians reporting timely access |
Increased number of Canadians reporting timely access (baseline is 80% of Canadians reporting timely access taken from the Health Services Access Survey, published in 2006) |
In 2009(**) 84.9% of Canadians, aged 12 and older, reported having a regular medical doctor, compared to 84.4% in 2008 and 84.9% in 2007. (*) The most recent figures from Statistics Canada show that most Canadians requiring routine or ongoing health services, health information or advice, and immediate care for a minor health problem do not report difficulties obtaining them. The percentage of Canadians self-reporting timely access to routine or ongoing health services was 82.8% in 2007 compared to 83.6% reported in 2003 and 2005.(*) In the 2007 survey, the percentage of Canadians self-reporting timely access to immediate care for a minor health problem was 74.7% compared to 79.3% in 2005 and 76.2 in 2003. The percentage of Canadians self-reporting timely access to health information or advice was 83.2% in 2007, compared with 85% in 2005 and 84.2% in 2003. |
| Percentage of Canadians satisfied with quality of primary, acute, chronic and continuing health care service | Increased number of Canadians satisfied with overall quality of health services (baseline is 85% of Canadians taken from Canadian Community Health Survey published in 2006) | In 2007, 85.2% of Canadians reported being "very satisfied" or "somewhat satisfied" with the way overall health care services were provided. Also, 89.8% of Canadians who received care from a physician reported being "very satisfied" or "somewhat satisfied" with the way physician care was provided. (*) |
| Increased sustainability of the health system through the development of new initiatives (long-term funding commitments, primary health care reform, use of science and technology) |
Increased number of initiatives that improve sustainability in the health system |
Initiatives relating to improved sustainability of the health care system included: |
Performance Data is from either:
(*) Healthy Canadians: A federal report on comparable health indicators, 2008 or
(**) Statistics Canada. Cansim Table 105-0501 - Health indicator profile, annual estimates, by age group and sex, Canada, provinces, territories, health regions (2007 boundaries) and peer groups, occasional,
CANSIM (database).
| Program Activity | 2008-09 Actual Spending |
2009-10 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Canadian Health System | 533.9 | 293.3 | 305.1 | 377.7 | 369.4 | Healthy Canadians |
| Canadian Assisted Human Reproduction | 3.9 | 1.5 | 1.5 | 2.6 | 2.6 | |
| International Health Affairs | 25.6 | 23.0 | 23.0 | 21.5 | 19.3 | |
| Total for SO 1 | 563.4 | 317.8 | 329.6 | 401.8 | 391.3 | |
| Performance Indicators | Targets | 2009-10 Performance |
|---|---|---|
| Increased rate of adherence to/compliance by industry with the Food and Drugs Act and its regulations, standards and guidelines (level of adherence/compliance of registered establishment by sector (e.g., meat, dairy, fish and seafood, processed food, shellfish and egg). |
Human drugs: 98% compliance; |
Human drugs: 96.0% compliance with the Food and Drugs Act Natural Health Products: baseline still to be established, as required. Medical Devices: An updated inspection program for medical devices, to be implemented in fall 2010, is expected to provide a measure of industry compliance with the Food and Drugs Act and regulations, standards and guidelines |
| Increased public confidence in available information related to health products, food and nutrition | 50% of Canadians are confident in the safety of the Canadian food supply (baseline data in 2006: 42%) |
A February 2010 survey conducted by Ekos regarding Canadians' knowledge and behaviour related to food safety indicates that 63% of Canadians are confident in Canada's food safety system. Over three in four say they feel they have enough information about food safety and how to protect themselves and their families from food-borne illnesses. |
| Program Activity | 2008-09 Actual Spending |
2009-10 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Health Products | 255.9 | 146.1 | 146.4 | 191.8 | 191.2 | Healthy Canadians |
| Food and Nutrition | 61.7 | 60.9 | 60.9 | 53.5 | 53.5 | |
| Total for SO 2 | 317.6 | 207.0 | 207.3 | 245.3 | 232.7 | |
| Performance Indicators | Targets | 2009-10 Performance |
|---|---|---|
| Number of incidents of deaths, exposures, illness, injury and adverse reactions. | Baseline information to be established in the next one to three years for defined populations. |
Until a new legislative framework for consumer products is in effect which imposes mandatory reporting, the number of consumer complaints is being used as an interim proxy performance indicator. Product Safety Complaints/Incidents showed an increasing trend: 2006-07, 567 complaints; 2007-2008, 672 complaints; 2008-2009, 944 complaints; 2009-2010, 1102 complaints. The increase in complaints by consumers is an indication of increased consumer awareness of risks associated with consumer products. Of the 1102 complaints received in 2009-2010, Health Canada met its service targets, responding to 100% of complainants and met its service standard following-up with 100% of companies. Depending on the severity of the incident reported, actions included product inspection with follow-up and enforcement actions, including recall or public advisory, as appropriate, and follow-up with the companies in question to ensure appropriate actions have been completed. |
| Proportion of regulatory actions addressed within service standards/targets. | To be set after baseline is established in 2011. |
Risk management actions were imposed on 100% of substances for which a significant risk was identified (20/20). Risk Management Instruments were developed for identified substances within expected timelines. 100% of human health risk assessments related to high priority federal contaminated sites were addressed within planned timelines. Screening assessment reports for Challenge and non-Challenge substances under the Chemicals Management Plan, were completed and published in the Canada Gazette Part I according to departmental timelines. |
| Percentage of inspected or verified registrants / firms / users compliant / non-compliant. | Baseline information to be established in the next one to three years for defined populations. | 84.3% of tobacco retailers are in compliance with regulations restricting underage youth from purchasing tobacco products, marking a significant increase from 69.8% in 2000. |
| Program Activity | 2008-09 Actual Spending |
2009-10 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Sustainable Environmental Health | 165.5 | 152.9 | 153.3 | 135.2 | 130.5 | Healthy Canadians |
| Consumer Products | 29.4 | 25.6 | 25.6 | 27.9 | 27.3 | |
| Workplace Health | 51.5 | 23.0 | 23.0 | 31.2 | 35.7 | |
| Substance Use and Abuse | 118.4 | 138.6 | 138.7 | 113.7 | 104.6 | |
| Pesticide Regulation | 64.5 | 45.1 | 45.1 | 54.1 | 49.5 | |
| Total for SO 3 | 429.3 | 385.2 | 385.7 | 362.1 | 347.6 | |
| Performance Indicators* | Targets | 2009-10 Performance |
|---|---|---|
| Life expectancy (at birth, by gender, on and off reserve), comparison of First Nations and Inuit with other Canadians | The Department will continue to work with others toward reducing these inequalities | Life Expectancy - The most recent data (2001) estimated life expectancy for First Nations at 70.4 years for males and 75.5 years for females; and for Inuit at 64.4 years for males and 69.8 years for females (Canadian average: males 77 years, females 82 years). |
| Birth weight (comparison of First Nations and Inuit with other Canadians) | Statistics from 2002-2003 indicate that 5.5% of First Nations on-reserve births are classified as low birth weight compared with 6.0% in Canada overall. The high birth weight rate for First Nations on-reserve is 21% approximately double the Canadian rate of 13%. Comparatively, the low birth rate among Inuit-inhabited areas (1999-2000) is 6.7% and the high birth rate is 13.1%. Health Canada is working in maternal and prenatal health to improve these outcomes. | |
| Mortality rates | Overall mortality for First Nations (2000) is 1.4x higher than for the Canadian population (1999) (based on age-standardized rates for regions with available data) | |
| Infant mortality rates | Reliable infant mortality data is currently not available. | |
|
Rates of conditions by type - e.g., diabetes, suicide, tuberculosis |
Diabetes Rates - 19.7% for First Nations on-reserve (most recent data 2002/2003) - 3.8 times higher than the Canadian average 3% in Inuit regions (most recent data 2005/2006) - below the Canadian average (5.1%) Suicide Rates - The rate of First Nations youth suicide (10 to 19 years) was 4.3 times greater than the Canadian average in 2000. The rate for Inuit regions (1999-2003) is 11.6 times higher than the Canadian average. Incidence of Tuberculosis - Registered Indians 5.9 times higher and Inuit regions 17.9 times higher than the general Canadian population (4.7 cases per 100,000 population |
*Note: Health Canada continues to work with its federal (e.g. Statistics Canada, Indian and Northern Affairs Canada) provincial and territorial partners as well as with First Nations and Inuit to improve the quality and accessibility of performance indicator data. Many indicators (e.g. life expectancy, mortality) only show changes over the very long-term.
| Program Activity | 2008-09 Actual Spending |
2009-10 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| First Nations and Inuit Health Programming and Services | 2,357.8 | 2,156.1 | 2,361.3 | 2,414.3 | 2,392.8 | Healthy Canadians |
| Total for SO 4 | 2,357.8 | 2,156.1 | 2,361.3 | 2,414.3 | 2,392.8 | |
| Program Activity | 2008-09 Actual Spending |
2009-10 | Alignment to Government of Canada Outcomes |
|||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| Internal Services* | 0.0 | 302.6 | 303.1 | 389.8 | 384.5 | |
| Total for Internal Services | 0.0 | 302.6 | 303.1 | 389.8 | 384.5 | |
*Note: Commencing in the 2009-2010 Estimates cycle, the resources for Program Activity Internal Services is displayed separately from other program activities; they are no longer distributed among remaining program activities, as was the case in previous Main Estimates. This has affected the comparability of spending and FTE information by Program Activity between fiscal years.
Contribution of Priorities to Strategic Outcome(s)
Health Canada applied the performance status rating as defined by Treasury Board of Canada Secretariat in their Guide to the Preparation of Part III of the 2010-11 Estimates.
- Exceeded - More than 100 per cent of the expected level of performance (as evidenced by the indicator and target or planned activities and outputs) for the expected result or priority identified in the corresponding RPP was achieved during the fiscal year.
- Met All - 100 per cent of the expected level of performance was achieved during the fiscal year.
- Mostly Met - 80 to 99 per cent of the expected level of performance was achieved during the fiscal year.
- Somewhat Met - 60 to 79 per cent of the expected level of performance was achieved during the fiscal year.
- Not Met - Less than 60 per cent of the expected level of performance was achieved during the fiscal year.
| Operational Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
I. Modernized safety framework: a) Continue implementation of Canada's Food and Consumer Safety Action Plan |
Ongoing |
Performance Status: mostly met a) The Department continued to work towards modernizing its legislative framework for parliamentary consideration, and has made strides to move regulatory activities forward. Continued regulatory oversight and guidance to industry was provided for health products by initiating pre-submission meetings intended to increase awareness and compliance with regulatory requirements. There was an increase in post-market surveillance activities and collaboration with stakeholders as well as an increase in voluntary adverse reaction reporting and an increase in post-market surveillance plans from industry. Health Canada has improved targeted consumer risk communication to increase public understanding of food safety risks and alert and safety systems. Health Canada continues to address areas of high risk and concern through ongoing targeted inspections, surveillance and compliance promotion under the existing legislation, and outreach to Canadians on the potential dangers associated with some consumer products. |
2 and 3 |
| b) Strengthen measures on tobacco control with respect to children and youth | Ongoing |
Performance Status: met all b) Bill C-32, Cracking Down on Tobacco Marketing Aimed at Youth Act, received Royal Assent in October 2009, and is expected to contribute to the reduced use of tobacco products by Canadian youth. |
2 and 3 |
| Operational Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
II. Strengthen First Nations and Inuit health programming: a) Stabilize First Nations and Inuit health system to support harmonization with provincial programs |
Ongoing |
Performance Status: met all a) Health Canada maintained its standards of care for First Nations and Inuit health programs and services. Canada's Economic Action Plan provided $67.4 million in 2009-2010 for the construction and renovation of health services infrastructure for First Nations, including health centres and nurses' residences. An additional investment of $134.5 million supported the Non-Insured Health Benefits program and the delivery of primary care nursing services in remote and isolated First Nations communities. The Aboriginal Health Transition Fund (AHTF) has improved integration of federally and provincially funded health services and adaptation of provincial and territorial health programs to meet the unique needs of First Nations and Inuit. This is occurring through the development of multi-partner joint service protocols, referral/discharge and information systems, collaborative committees, and governance structures and/or processes. |
4 |
| b) Continue integration of federal/provincial/ territorial First Nations health programs and services through tripartite agreements | Ongoing |
Performance Status: met all b) Health Canada, the British Columbia government and the British Columbia First Nations Leadership Council continue to work toward implementation of the commitments made in the 2007 Tripartite First Nations Health Plan. Discussions among partners regarding a 10-year Saskatchewan Health and Wellness Plan are ongoing. |
4 |
| Operational Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
III. Health system innovation: Continue to work with the provincial/territorial governments on health human resources and other matters of national interest through focussed and innovative means |
Ongoing |
Performance Status: mostly met Working in collaboration with provincial and territorial governments, Health Canada supported the development and promotion of innovative ideas that can result in improved access, effectiveness and efficiency for the Canadian health care system. $20 million annually has been invested in the Pan-Canadian Health Human Resource Strategy to ensure the availability of appropriate, skilled, competent health professionals. Initiatives also include strategies to facilitate the integration of internationally-educated health professionals into Canada's health system and for demonstration projects designed to improve retention and recruitment of nurses. The Department is accelerating the implementation of Health Information Systems, via Canada Health Infoway, to support the continued implementation of electronic health records and other electronic health technologies (e.g. telehealth and public health surveillance). Health Canada is also providing advice and active support to the Canadian Institutes of Health Research led Drug Safety and Effectiveness Network The Department supported all provincial and territorial governments in progress toward establishing Patient Wait Times Guarantees (PWTGs) in at least one of the priority clinical areas with funding through the three-year PWTG Trust and the PWTG Pilot Project Fund, both of which ended March 31, 2010. PWTG pilot projects were completed in eight jurisdictions. By April 2010, nine of ten provinces had established guarantees with the remaining province and three territories indicating they would do so later in 2010. A March 2010 Canadian Institute for Health Information study shows that most patients are now receiving care within recommended wait times for priority procedures: hip fracture repairs or replacements, cataract surgery, and cancer radiation therapy. |
1, 2 and 3 |
| Management Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
IV. Increase quality and coherence of strategic policy: a) Talent Management Framework |
Ongoing |
Performance Status: mostly met a) The Health Canada Talent Management Strategy, an initiative for maximizing the Department's investment in human resources at all levels and all areas of expertise, proceeded on schedule, although fiscal pressures to meet costs related to H1N1 and required budget reductions led to reallocations that delayed some elements of the strategy. |
1, 2, 3 and 4 |
| b) Ensure all policy is evidence-based by better integrating science/research in the policy development process | Ongoing |
Performance Status: met all b) A Health Canada Science Plan was developed to strengthen links between science and decision-making in the Department. Based on extensive consultations, department-wide science needs have been identified to establish science priorities, as well as priorities for policy work and related evidence gathering and analysis over the longer term. Centres of Expertise were established to provide guidance within the Department, for: nanotechnology, science and technology foresight, bioethics, and risk assessment. A Science Excellence Framework was also developed. |
1, 2, 3 and 4 |
| Management Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
V. Enhance corporate processes for increased accountability: a) Strengthen integrated planning b) Improve performance measurement and indicators |
Ongoing |
Performance Status: met all a) Through continual process and technology improvements, departmental operational planning has begun integrating business plans with financial, HR, IT, investment planning and facilities management. Performance Status: met all b) A review was conducted on Health Canada's Program Activity Architecture and work began to update this structure and to develop a Performance Measurement Framework for implementation with the 2011/2012 planning cycle. The revised PAA will include updated performance indicators that will improve the objective basis for evaluating the performance of programs. |
This management priority is part of the Internal Services Program Activity which contributes to all strategic outcomes |
|
c) Enhanced Financial Management Control Framework |
Ongoing |
Performance Status: met all c) The Department incorporated a series of measures to equip its staff to manage financial risks, by: raising awareness; providing appropriate knowledge and tools; training and development in financial management; and, by documenting main business processes and key risk and control points to support the management and oversight of its control systems. In preparing for auditable financial statements, the Department completed the documentation of key business processes and related internal controls over financial reporting. |
This management priority is part of the Internal Services Program Activity which contributes to all strategic outcomes |
| Management Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
VI. Increase transparency and innovative engagement with Canadians a) Strengthen departmental frameworks and policies for engaging Canadians |
Ongoing |
Performance Status: met all a) Work continued toward a Departmental Action Plan to support better integration of fundamental public involvement principles on openness/transparency/accountability in departmental decision making. An implementation plan to ensure the consistent understanding and application of a departmental Consumer Information Strategy was developed for implementation in the new fiscal year. New software tools to track general consumer inquiries phone calls and e-mails about regulated products were put in place to allow us to measure call volume and improvements in response time. Health Canada used social media tools that provide access to information for consumers, health professionals and industry when, where and how they want it. |
1, 2 and 3 |
| b) Better communication with Canadians and our stakeholders, and improve public's access to health and safety information | Ongoing |
Performance Status: met all b) Health Canada made strides in making food, health and consumer product information more accessible, credible and more consumer friendly, for example:
|
1, 2 and 3 |
Risk Analysis
Over the last fiscal year, a number of risks were faced by the Department and needed to be managed in order to achieve the Department's mandate and strategic objectives. Also, there were three major external incidents that influenced the year's events for Health Canada. The first was the pace of progress on the Food and Consumer Safety Action Plan. In particular, the legislative process surrounding Bill C-6, the proposed Canada Consumer Product Safety Act, did not receive Royal Assent. Without the Royal Assent necessary for the Department to proceed on key changes, it was not possible to deliver all the expected results for the year.
The second event was the emergence of H1N1 influenza in April 2009. Health Canada management shifted much of its focus, and substantial resources, to the work necessary to understand and address H1N1 in Canada and to work with partners on international aspects of the H1N1 response. Health Canada reallocated resources from lower-priority commitments to ensure that a new vaccine would be available for all Canadians and emergency interventions could be improved. Joint measures were conducted in partnership with the Public Health Agency of Canada to ensure a coordinated response to national health risks and protect the well-being of Canadians.
The Department took similar action to support the Government in addressing the impact on access to medical isotopes after the shutdown of the Chalk River nuclear reactor. Alternative sources of isotopes around the world were identified and used by provincial and territories health establishments to secure isotope supplies, while the Department also identified the value of planning for similar medical situations in ways that take into account the complex interplay of medical, social and business interests.
Beyond that, other elements of the risk analysis set out in the RPP were managed during the year. Health Canada applied the lessons learned from the 2008 listeriosis outbreak. This led to actions such as a revision of roles between organizations and evaluation of options to increase laboratory capacity and access. In collaboration with the Canadian Food Inspection Agency (CFIA) and the Public Health Agency of Canada (PHAC), public health officials and provincial and territorial Ministries of Health, Health Canada revised its policy on Listeria monocytogenes in ready-to-eat foods that would have impacts on the Canadian Food Inspection Agency, provincial/territorial governments and food industry as they identify steps to reduce the risk of Listeria contamination in these foods. Health Canada briefed the medical community, public health officials, the food industry and the public on matters related to listeriosis, and participated in public awareness campaigns about safe food practices.
Health Canada recognized the risks associated with the growing expectation and need for information from the public in a context where the information is globalized and made available 24 hours a day, and where science and technology rapidly evolve. For example, the Department supported the development and dissemination of health knowledge and information through the funding for the Canadian Institute for Health Information; by ensuring a consistent approach to communicating risks and benefits of regulated products; and by dedicated resources to better explain health risks to Canadians.
In a context of declining fiscal flexibility for the Government of Canada, the Department acknowledged that financial integrity of key programs could be at risk, considering for example challenges from increasing costs of its regulatory activities, outdated user fee regimes, and the ongoing need to support First Nations and Inuit health services. To ensure the sustainability of key programs: Health Canada reallocated funds to align with priorities; conducted monthly financial reviews to manage resources effectively; moved to secure increased cost-recovery revenues through new user fees proposals; and obtained additional funding for First Nations and Inuit health programs and benefits.
Health Canada addressed risks associated with managing horizontal initiatives such as the Chemicals Management Plan, Clean Air Agenda, and Food and Consumer Safety Action Plan. In an effort to increase engagement with external partners, Health Canada built on and clarified existing roles, responsibilities and accountabilities in order to enhance collaboration and achieve outcomes. Lessons in optimizing horizontal external relationships will be important as the Department moves forward in its ongoing effort to support collaboration among federal, provincial and Aboriginal partners. These collaborative efforts support the improvement of health services for First Nations through enhanced integration and alignment of federal and provincial health systems as well as increased First Nations and Inuit capacity to design, deliver and manage their own health programs.
The Department also addressed risks associated with its internal management. Committed to develop policy based on cutting-edge science, the Department addressed associated risks through initiatives such as creation of a Science and Policy Integration Unit, a new Science and Policy Round Table and the Health Canada Science Forum. Health Canada also implemented initiatives to attract and retain key talent in the face of a competitive labour market and human resource challenges such as an aging work force, a high rate of staff eligible for retirement, the need to staff positions in remote locations and the need to respect official language commitments. The Department also continued to implement a reorganization that has addressed regional decision-making and accountability challenges.
Expenditure Profile
For the 2009-10 fiscal year, Health Canada spent $3,748.9 million to meet the expected results of its program activities and contribute to its strategic outcomes.
The figure below illustrates Health Canada's spending trend from 2007-2008 to 2009-2010.
Spending Trend
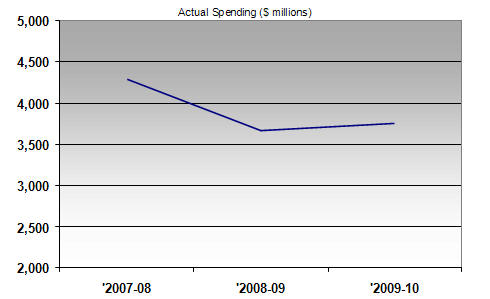
For the 2007-2008 to 2009-2010 periods, the total spending includes all Parliamentary appropriation sources: Main Estimates, Supplementary Estimates, Treasury Board collective bargaining, operating budget carry forward, and other special adjustments.
In 2007-08, actual spending was particularly high due to the $1 billion compensation payments to individuals infected with the Hepatitis C virus through the Canadian blood supply before 1986 and after 1990.
The table below offers a comparison of the Main Estimates, planned spending, total authorities and actual spending for the most recently completed fiscal year, as well as the historical actual spending figures for the previous year.
| Program activities | 2008-2009 Actual Spending |
2009-2010 Main Estimates |
2009-2010 Planned Spending |
2009-2010 Total Authorities |
2009-2010 Actual Spending |
|---|---|---|---|---|---|
|
Canadian Health System |
533.9 | 293.3 | 305.1 | 377.7 | 369.4 |
|
Canadian Assisted Human Reproduction |
3.9 | 1.5 | 1.5 | 2.6 | 2.6 |
|
International Health Affairs |
25.6 | 23.0 | 23.0 | 21.5 | 19.3 |
|
Health Products |
255.9 | 146.1 | 146.4 | 191.8 | 191.2 |
|
Food and Nutrition |
61.7 |
60.9 | 60.9 | 53.5 | 41.5 |
|
Sustainable Environmental Health |
165.5 |
152.9 | 153.3 | 135.2 | 130.5 |
|
Consumer Products |
29.4 | 25.6 | 25.6 | 27.9 | 27.3 |
|
Workplace Health |
51.5 | 23.0 | 23.0 | 31.2 | 35.7 |
|
Substance Use and Abuse |
118.4 | 138.6 | 138.7 | 113.7 | 104.6 |
|
Pesticide Regulation |
64.5 | 45.1 | 45.1 | 54.1 | 49.5 |
|
First Nations and Inuit Health |
2,357.8 | 2,156.1 | 2,361.3 | 2,414.3 | 2,392.8 |
|
Internal Services |
0.0 | 302.6 | 303.1 | 389.8 | 384.5 |
| Total Department |
3,668.1 |
3,368.7 |
3,587.0 |
3,813.3 |
3,748.9 |
Note: Commencing in the 2009-10 Estimates cycle, the resources for Program Activity: Internal Service is displayed separately from other program activities; they are no longer distributed among the remaining program activities, as was the case in previous Main Estimates. This has affected the comparability of spending and FTE information by Program Activity between fiscal years.
The $218.3 million increase from Main Estimates to Planned Spending is due to anticipated funding from the Government's Economic Action Plan to stabilize the Non-Insured Health Benefits program and primary care services and a direct investment for construction and renovation of infrastructure for First Nations and Inuit health services, as well as anticipated additional funding relating to the Official Languages Health Contribution Program.
The $226.3 million increase from Planned Spending to Total Authorities is due to new program initiatives received through Supplementary Estimates, including funding for addressing the first and second wave of the H1N1 flu virus outbreak, for providing mental health and emotional support services and the administration and research required to support the federal government's obligations under the Indian Residential Schools Settlement Agreement, and for addressing the submission review backlog in the Natural Health Products Program.
The $64.4 million difference between Total Authorities and Actual Spending was mainly the result of lapses in TB special purpose allotments for H1N1, the Indian Residential Schools Settlement Agreement, and Health Council, as well as in the TB frozen allotment for the National Anti-Drug Strategy (Mandatory Minimum Penalties).
Canada's Economic Action Plan (CEAP)
Health Canada was allocated $211.9 M in 2009-2010, for initiatives under Canada's Economic Action Plan (CEAP). They are:
- $0.3 M for a one-year extension for Canadian Environmental Sustainability Indicators;
- $134.5 M to strengthen the Non-Insured Health Benefits program and enhance support for primary care services for First Nations and Inuit;
- $67.4 M for infrastructure investments through the Health Facilities and Capital Program for First Nations and Inuit;
- $9.0 M for investments in the maintenance and modernization of Health Canada laboratories;
- $0.7 M for maintenance or upgrading of existing Arctic research facilities (facilities transferred from INAC to HC in 2009-2010).
In addition, $500 M announced in the 2009 Budget and confirmed in Budget 2010, will be provided to Canada Health Infoway, which will be governed by the terms and conditions of a new agreement.
Departamental Spending Trend
($ millions)
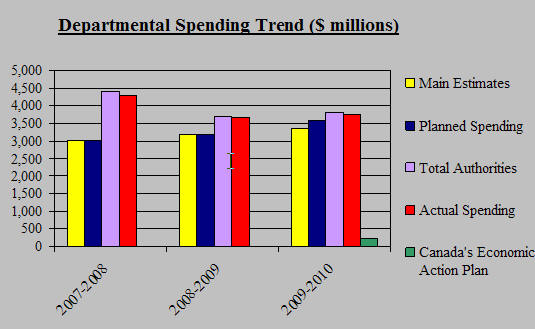
Voted and Statutory Items
The table below illustrates the way in which Parliament approved Health Canada's resources in 2008-09 and 2009-10 and shows, for 2009-10, changes in resource levels from planning to Main Estimates to final authorities, as well as the actual spending at year-end.
| Vote | 2008-2009 Actual Spending |
2009-10 Main Estimates |
2009-10 Planed Spending |
2009-10 Total Authorities |
2009-10 Actual Spending |
|---|---|---|---|---|---|
| Health Canada | |||||
| (1) Operating expenditures |
1,884.7 |
1,788.4 |
1,896.2 |
2,016.1 |
1,967.7 |
| (5) Capital expenditures |
40.9 |
40.8 | 41.6 | 53.5 | 47.0 |
| (10) Grants and contributions |
1,389.6 |
1,422.7 |
1,529.2 |
1,528.2 |
1,519.2 |
| (S) Minister of Health - Salary and motor car allowance | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 |
| (S) Spending of proceeds from the disposal of surplus Crown Assets | 0.1 | 0.0 | 0.0 | 0.9 | 0.4 |
| (S) Refunds from Previous Years Revenue | 0.2 | 0.0 | 0.0 | 0.9 | 0.9 |
| (S) Canada Health Infoway Inc | 123.0 | 0.0 | 0.0 | 64.9 | 64.9 |
| (S) Transfer payments to Mental Health Commission of Canada | 110.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| (S) Contributions to employee benefit plans |
119.5 |
116.7 |
119.9 |
139.8 |
139.8 |
| (S) Payments in connection with the Patent Act (Patented Medicines) | 0.0 | 0.0 | 0.0 | 9.3 | 9.3 |
| Total Department |
3,668.1 |
3,368.7 |
3,587.0 |
3,813.3 |
3,748.9 |
(S) Denotes statutory items which do not require an appropriation act
Section II - Analysis of Program Activities by Strategic Outcome
Strategic Outcome 1 - Accessible and sustainable health system responsive to the heath needs of Canadians
Maintaining the accessibility and sustainability of Canada's health system is a shared responsibility requiring Health Canada to work closely with provincial and territorial governments, as well as health organizations and other stakeholder groups. With Health Canada playing a significant role, the Department continually examines new and innovative approaches and responses to the health priorities and needs of Canadians.
Serving as a partner, an enabler, an innovator, a knowledge broker and a proponent of transparency and accountability, Health Canada plays a role in supporting the sustainability of Canada's health system. To Canadians, sustainability means the availability, maintenance and advancement of key attributes of Canada's publicly funded health system such as accessibility, efficiency and effectiveness. In the face of perpetually shifting and growing health system demands, the Department develops policies in support of a sustainable health system for Canadians.
This program activity provides strategic policy advice on health care issues such as improved access, quality and integration of health care services to better meet the health needs of Canadians, wherever they live or whatever their financial circumstances. The objective is pursued mindful of long-term equity, sustainability and affordability considerations and in close collaboration with provinces and territories, health professionals, administrators, other key stakeholders and citizens.
This program activity benefits Canadians by contributing to improved access, quality and integration of health services. This is achieved through investments in the health system and in health system renewal; for instance by reducing wait times for health care services, by working with provinces and territories to ensure that the principles of the Canada Health Act are respected, by developing health information and health measures for Canadians, by meeting the health and health access needs of specific groups, such as official language minority communities, and by ensuring the implementation of agreements between federal/provincial/territorial ministers of Health.
| Expected Results |
Performance Indicators |
Targets | Performance Status |
Performance Summary |
|---|---|---|---|---|
| Improved health care system planning and performance, including wait times reduction | Reports and analyses related to issues such as wait times reduction, health human resources planning, and provision of chronic, palliative and continuing care are used to improve the health care system | Increased awareness and knowledge of new approaches, models and best practices related to health care renewal | mostly met |
Completed Patient Wait Times Guarantees Pilot Projects in eight jurisdictions. Patient Wait Times Guarantees in place in nine provinces, supported by the federal Patient Wait Times Guarantee Trust. First Nations communities implemented pilot projects in 10 sites to test Patient Wait Time Guarantee for prenatal and diabetes services. Investments through the Pan-Canadian Health Human Resource Strategy assisted with: the managing of health care providers; using HR skills effectively; implementing healthy, supportive, learning workplaces; and effectively planning and forecasting health human resources. Developed tools, through financial support, to facilitate the integration of internationally educated health professionals into the Canadian health care system. Facilitated, through funding, a Roundtable on the Cost-Effectiveness of Chronic Disease Management Programs to increase participants' understanding and knowledge of the costs and benefits of chronic disease management programs across Canada. Provided funding: to translate palliative and end-of-life caregiving resources for Chinese Canadians and First Nations; apply national quality standards to palliative and end-of-life care given by volunteers; promote knowledge transfer of palliative and end-of-life care to the public; and broaden human resources capacity to deliver palliative and end-of-life care. |
| Enhanced capacity of governments and stakeholders to support health system planning | Governmental and stakeholder engagement activities (e.g., meetings, workshops, conferences, program and policy proposals) | Increased collaboration and consultation between governments and stakeholders to advance key health care issues | mostly met |
Continued to co-chair the F/P/T Advisory Committee on Health Delivery and Human Resources to support pan-Canadian collaboration on HHR challenges, including consultation on future Internationally Educated Health Professionals Initiative investments. Support for FPT eHealth collaboration through funding for Canada Health Infoway . Worked with the Canadian Institutes of Health Research toward the establishment of the Drug Safety and Effectiveness Network (DSEN), the staffing of a DSEN Executive Director, and the development of a DSEN Performance Measurement and Evaluation Framework. DSEN partners engaged international partners implementing related initiatives, (e.g. EnCepp in EU , Sentinel in US) to share best practices and explore opportunities for data sharing. Hosted a work session on Healthcare Technology Management on optimal use of health technologies in the healthcare system. |
| Awareness and understanding among health sector decision-makers and the public of the factors affecting accessibility, quality and sustainability of Canada's health-care system and the health of Canadians | Publication of information that raises awareness and understanding of the factors affecting accessibility, quality and sustainability of Canada's health-care system and the health of Canadians | Timely and accessible health research and information on priority health issues available to Canadians | mostly met |
A new Healthy Canadians report on health system performance and population health status offered more indicators and improved interpretive information, in response to recommendations by the Commons Standing Committee on Health and the Auditor General. The Health Policy Research Bulletin highlights policy research on themes relevant to the Federal Health Portfolio, with the objective of strengthening the evidence base for decision making. Issue 16 of the Bulletin on "Regulatory Modernization: Reshaping Canada's Health and Safety Systems for Food, Health and Consumer Products" was released in March, 2010 A Science Colloquium on the Health of Canada's official language minority communities focused on health research for official language minority communities. |
Canada's Economic Action Plan (CEAP)
Canada Health Infoway
Canada's Economic Action Plan allocated $500 million to Canada Health Infoway (Infoway) to support the goal of establishing Electronic Health Records for Canadians, to speed up the implementation of Electronic Medical Records in physicians' offices, and to integrate points of service, such as hospitals, pharmacies and community care facilities.
The Auditor General's Report of Fall 2009 featured a chapter on electronic health records and made recommendations to promote enhanced accountability in relation to Infoway's investments in electronic health records. Monitoring Infoway's response to this report provided the federal government with one source of information leading to the completion of due diligence required for the release of these funds, as confirmed through Budget 2010. A new funding agreement between Infoway and Health Canada has been put in place to govern the use of the new allocation, which enables Infoway to draw annually on these funds.
Performance Summary and Analysis
Above and beyond the policy leadership and research support that Health Canada provides for health care system improvements under this program activity, there were four major areas of attention. One was the ongoing support for the Government's Patient Wait Times Guarantee (PWTG) commitment. The Department supported all provincial and territorial governments in progress toward establishing PWTGs by March 2010 in at least one of the priority clinical areas (cancer treatment, heart procedures, diagnostic imaging, joint replacement and sight restoration) with funding through the three-year PWTG Trust and the PWTG Pilot Project Fund, both of which ended March 31, 2010. By April 2010, nine of ten provinces had established guarantees, with the remaining province and three territories indicating they would do so later in 2010. A March 2010 Canadian Institute for Health Information study shows that most patients are now receiving care within recommended wait times for priority procedures: hip fracture repairs or replacements, cataract surgery, and cancer radiation therapy.
A second area of attention was the effort to address Canada's health human resource needs. Health Canada's work continued to support the integration of internationally educated health professionals into the Canadian health care system. In particular, support was provided for 11 multi-year provincial and territorial agreements encompassing over 60 projects and six pan-Canadian agreements, including the development of an assessment tool for International Medical Graduates. Health Canada also continued to collaborate with provinces, territories and health system partners to improve the planning and management of health human resources through funding for 39 projects in the following areas: health care providers; effective use of human resources skills; healthy, supportive, learning workplaces; and effective planning and forecasting of health human resources. As an example, one project conducted a comprehensive review of physician education in Canada , and assessed current and future societal needs, to better align the medical education curriculum with population health needs. All governments are learning and sharing best practices as a result of collaborative efforts and knowledge exchange.
The third area of attention was our commitment to work with official language minority communities on their health system priorities. Under the Official Languages Health Contribution Program, we increased the number of health professionals able to provide services in official language minority communities. In 2008-2009, the post-secondary institutions member of the Consortium national de formation en sant� had 404 new francophone graduates in the health professions, such as medical doctors, nurses, nurses' aides, physiotherapists, and radiology technicians. In 2009-2010, Health Canada funded 965 new students in 87 health disciplines. Between 2003 and 2009, Health Canada funding has supported the graduation of 1721 francophone health professionals.
A final area was our support for the continued development of electronic health technologies led by Canada Health Infoway, in collaboration with provinces and territories. As noted in Canada Economic Action Plan, i n 2009-2010, Infoway established a Patient Access to Quality Care (PAQC) investment program to support innovative jurisdictional demonstration projects that will facilitate improved access to quality care and reduced wait times.
This program activity implements the Assisted Human Reproduction Act, which seeks to protect and promote human health, safety, dignity and human rights in the use of Assisted Human Reproduction (AHR) technologies. It develops policies and regulations in the area of assisted human reproduction. The science of AHR is evolving rapidly and, as a result, the program activity engages stakeholders on an ongoing basis to find a balance between the needs of patients who use these technologies to help them build their families, the children born from these technologies and the providers of these services with health and safety as the overriding factors. The goal of the policies and regulations is to develop a responsive regulatory regime which is a leader both domestically and in the international AHR community, and reflects the objectives put forward in the Assisted Human Reproduction Act. The program activity gathers input from stakeholders, including the provinces, to ensure a pan-Canadian approach. Once implemented, the benefits from this program for Canadians will be realized when the needs of patients who use these technologies to help them build their families, the children born from these technologies, and the providers of these services, are balanced with health and safety as the overriding factors.
| Expected Results |
Performance Indicators |
Targets | Performance Status |
Performance Summary |
|---|---|---|---|---|
| Increased input of Canadian stakeholders on assisted human reproduction technologies | Stakeholder and advisory panel involvement and engagement | Increased stakeholder coordination and consultation support and advance regulatory development | somewhat met | Stakeholder advisory panels were engaged on an ad-hoc individual basis, however consultations were scaled back in light of the Supreme Court of Canada process. |
| Increased knowledge of the application of assisted human reproduction procedures in Canada | Monitoring, collection, and analysis of relevant and current information in assisted human reproduction practices leading to the development of evidence-based policy documents | Improved monitoring and awareness of assisted human reproduction practices | mostly met | Information related to AHR practices and stakeholders was collected. |
|
Increased number of assisted human reproduction regulations to protect the health and safety, dignity, and rights of Canadians using assisted human reproduction technologies Health and safety risks related to assisted human reproduction technologies addressed |
Reports and supporting documentation on relevant issues addressed through appropriate regulations and other instruments developed to enforce the AHR Act | AHR regulations and other instruments | not met | On hold pending outcome of the Supreme Court of Canada process. |
Performance Summary and Analysis
The Department's ability to develop policies and regulations continues to be delayed because a constitutional challenge to parts of the Act is before the Supreme Court of Canada. For example, the Department delayed the prepublication of draft regulations and supporting activities that could be affected by the challenge until it is resolved. However, Health Canada did make progress where it could, such as the further development of some regulatory policy and potential regulatory frameworks. Significant work was accomplished on policy development for "third party" donors, including screening and testing.
Health Canada works internationally through leadership, partnerships and collaboration to fulfill its federal mandate of making Canada's population among the healthiest in the world. International Affairs serves as the Department's focal point to initiate, coordinate, and monitor departmental policies strategies and activities that help promote Canadian priorities and values on the international health agenda. International collaboration on global health issues provides an important benefit for Canadians given that the health of Canadians is influenced significantly by public health risks originating from other countries. Global issues such as pandemic influenza preparedness, HIV/AIDS strategies and global health security are addressed with key external health partners such as the World Health Organization (WHO) and the Pan American Health Organization (PAHO).
Countries and international organizations want to connect quickly to information about Canada's health care system and initiatives. This program activity strives to share Canada's best policies and practices with other countries, and assists in the development of bilateral agreements with numerous countries on important health issues. This program activity delivers strategic policy advice on international health issues to the Minister of Health, senior management and the Health Portfolio, including appropriate representation at international fora concerning the health portfolio. It also manages grants to non-profit organizations for projects in the domain of international health that are aligned with Canada's priorities in global health.
| Expected Results |
Performance Indicators |
Targets | Performance Status |
Performance Summary |
|---|---|---|---|---|
| Increased knowledge and understanding of current and emerging international health issues; | Strategic engagement with stakeholders and other governments (e.g. consultations and outreach activities with key stakeholders and international partners) | Increased awareness and knowledge of new approaches, models and best practices related to international health priority issues | met all | Contacts with other countries and in multilateral organizations, such as the Pan American Health Organization (PAHO), World Health Organization (WHO), the Organization for Economic Co-operation and Development (OECD) and Asia-Pacific Economic Cooperation (APEC) advanced Canada's priorities on issues such as: regulatory cooperation, pandemic influenza preparedness, H1N1 and global health security. |
|
Enhanced multilateral, bilateral, regional and intersectoral collaboration on current and emerging international health issues of priority to Canada; |
Number of new collaborations with key stakeholders on current and emerging international health issues of priority to Canada | Increased strategic engagement in international meetings, conferences and fora; and an increased number of Canadian representatives on the boards or committees of key international health organizations |
mostly met |
Officials participated in a wide variety of committees, boards and meetings for multilateral organizations listed above and others. Health Canada engaged in close collaboration on H1N1 with international partners to share information and coordinate pandemic response strategies - including through the Global Health Security Initiative, an informal partnership of G7 countries, Mexico, the European Commission and WHO. Health projects in over 60 countries were sponsored by the Department, as a member of the Global Health Research Initiative. Facilitated 6 outgoing and 17 incoming visits from representatives of countries including China, Morocco, Brazil and Japan to learn and share information about issues such as health care, food safety, eHealth and H1N1. Five international policy dialogues facilitated the exchange of information and innovative practices, an increase from two dialogues in 2008-2009. |
|
Influence the international health agenda in a manner that supports Canada's health priorities, foreign policy and development objectives. |
Number of multilateral, bilateral negotiations or agreements that Health Canada leads or supports in order to advance Canada's health priorities | An increase in the number of resolutions or policy positions introduced by Health Canada which reflect Canadian priorities, and policy objectives and an increase in the number of international agreements, treaties or memoranda of understanding which advance Canada 's health priorities | mostly met |
Successful negotiation and passing of resolutions including 16 at WHO, 22 through PAHO and 18 in other United Nations forums. Contributions to governance and policy documents of international organizations (e.g. the Framework Strategy for Cooperation with PAHO). |
Performance Summary and Analysis
Under this program activity, Health Canada actively engaged in the development of international health policies, standards and actions that help promote Canadian priorities and values, and built international consensus to promote global health security and address health issues such as pandemic influenza preparedness, food and consumer product safety during 2009-2010.
In addition to the ongoing responsibilities related to work with other governments and with international organizations with health mandates that are indicated in the table above, this program activity was affected significantly by the H1N1 issue. It was the focal point for Health Canada's international contact and collaboration as partners worked together to share information and improve responses to H1N1. Collaborations of this nature increase trust and understanding between international jurisdictions, laying the foundation for improved future cooperative ventures.
Strategic Outcome 2 - Access to Safe and Effective Health Products and Food, and Information for Healthy Choices
Under this strategic outcome, Health Canada is committed to promoting and protecting the health and safety of Canadians by working towards reducing health risks from health products and food and by providing information so Canadians can make informed decisions and healthy choices.
As the federal authority responsible for the regulation of health products and food, Health Canada evaluates and monitors the safety, quality and efficacy of health products as well as the safety and nutritional quality of food. The Department also promotes the health and well-being of Canadians through a broad range of activities related to health products and food, including developing
nutrition policies and standards such as Canada's Food Guide and information to the public in newsletters such as It's Your Health.
The Health Products program activity is responsible for a broad range of health protection and promotion activities that affect the everyday lives of Canadians. Under the authority of the Food and Drugs Act and Regulations, and the Department of Health Act, this program activity benefits Canadians by evaluating and monitoring the safety, quality and effectiveness of drugs (human and animal), biologics, medical devices and natural health products, and conducts surveillance, compliance and enforcement activities. This program activity also provides timely, evidence-based and authoritative information to stakeholders (including but not limited to: health care professionals such as physicians, pharmacists and practitioners such as herbalists, naturopathic doctors and Traditional Chinese Medicine practitioners) and members of the public to enable them to make informed decisions and healthy choices.
| Expected Results |
Performance Indicators |
Targets | Performance Status |
Performance Summary |
|---|---|---|---|---|
|
By 2013, implementation of the five-year Food and Consumer Action Plan Reduced exposure to health Risks related to Health Products |
Number of reports on pharmacovigilance plans (PvR) received Number of Risk Management and Mitigation Plans (RMP) received |
By 2013, increasing trend in reported pharmacovigilance plans By 2013, increasing trend in reported Risk Management and Mitigation Plans |
met all |
Pharmacovigilance plans and Risk Management and Mitigation Plans have been merged into one indicator as both indicators are concerned with risk and the activities are almost identical in nature except in relation to when the processing takes place. 57 PvR/RMP received (Pharmaceuticals and Biologics/Radiopharmaceuticals only) up from 18 in 2008-2009. |
|
Increased ability to monitor and identify safety concerns before they arise |
Number of pre-submission meetings held per year |
An equal amount or an increase in pre-submission meetings for biologics and radiopharmaceuticals in 2009-2010. An equal amount or an increase in pre-submission meetings for pharmaceuticals drugs for 2009-2010. |
mostly met |
59 pre-submission meetings were held with industry for biologics and radiopharmaceuticals (65 in 2008-2009 / 56 in 2007-2008) 50 pre-submission meetings were held with industry for pharmaceutical drugs (96 in 2008-2009). Workload pressures and a focus on critical meetings resulted in a reduction of pre-submissions meetings. Written responses were substituted wherever appropriate. |
| Number of Product Monographs made available to the public | In 2009-2010 estimated posting of 2000 Product Monographs on the Health Canada website | met all |
1985 product monographs were posted and 168 natural health product monographs have been published to date. 100% of product monographs for new drug submissions were posted. |
|
| Increased industry awareness and knowledge of regulatory requirements | Number of firms inspected that are compliant with Good Manufacturing Practices requirements for Active Pharmaceutical Ingredients | By 2013, an increase in the number of firms inspected that are compliant with Good Manufacturing Practices for Active Pharmaceutical Ingredients (API) | n/a |
No inspections were conducted as the API regulatory framework was not yet in place. Activities continued at the research, planning, training and program level. Major emphasis was placed on confirming the current API landscape in Canada and filling the gaps in inspector API knowledge. |
|
Increased knowledge of post-market drug safety and effectiveness to inform decisions |
Number of Centres/ Partners participating in the Drug Safety and Effectiveness Network (DSEN) |
Drug Safety and Effectiveness Network coordinating infrastructure to be established in 2009-2010 Ten centres/partners participating in Drug Safety and Effectiveness Network by 2011-2012 |
met all |
Appointment of the DSEN Executive Director, at the Canadian Institutes of Health Research, completed the establishment of the coordinating infrastructure. On track to target. |
| Safer use of health products by consumers and health professionals | Number of consumers aware of risks associated with health products imported for personal use | By 2013, more consumers aware of risks associated with the import of non-compliant health products | mostly met | This indicator is currently under review, due to public opinion research constraints, and is likely to be modified in the coming year. |
| Enhanced capacity of Health Canada and industry to identify and respond to risk issues | Percentage of hospitals compliant with mandatory adverse reaction reporting | By 2013, increasing trend in reported adverse reactions from hospitals | exceeded | Adverse Reaction reports received increased 20% over 2008-2009. Note: Under current legislation, all adverse reaction reporting is voluntary. |
| Number of Periodic Safety Update Reports (PSUR) received | By 2013, increasing trend in reported Periodic Safety Update Reports | met all |
175 PSURs received (127 in 2008-2009). This increasing trend demonstrates enhanced program awareness. |
Performance Summary and Analysis
Under its mandated responsibilities for regulating under the Food and Drugs Act, the Department regulated the safety, efficacy and quality of health products (pharmaceuticals, biologics, medical devices, natural health products and veterinary drugs) before they were authorized for sale on the Canadian market.
In addition to the above, the Department focused on implementing those aspects of the five-year Food and Consumer Safety Action Plan that could be done within the existing regulatory framework. At the same time, Health Canada worked towards modernizing the current regulatory framework under the Food and Drugs Act for eventual parliamentary consideration, which will also be necessary to support some of the performance indicators and targets listed in the table above, particularly those with lower status ratings.
Continued regulatory oversight and guidance to industry was provided as evidenced by the number of manufacturing pre-submission meetings intended to increase awareness and compliance with regulatory requirements. The increased volume and complexity of submissions for pharmaceutical drugs resulted in delays in completing some reviews. However, significant progress was made to reduce submission backlogs for natural health products. T here was an increase in both post-market surveillance activities and collaboration with stakeholders. An increasing trend in voluntary adverse reaction reporting as well as in pharmacovigilance plan submissions from industry was also noted.
More product specific information was made available to the public through the drug database and through the MedEffect e-Notice, resulting in improved access for Canadians to information about advisories, recalls and warnings for commonly-used health products. A new National Border Integrity Program was put in place to protect Canadians from health concerns related to imported and exported health products.
Management of this program activity continued during a number of emerging high-profile issues requiring departmental attention, particularly the medical isotope shortage and H1N1 influenza in Canada. Health Canada's pandemic preparedness and response activities included close collaboration with the Public Health Agency of Canada, other national regulatory authorities and the World Health Organization. Collaboration with other regulatory authorities lead to exchange of information in real time, which enabled Health Canada to maximize the amount of data available to support timely authorization of pandemic products, such as the H1N1 vaccine.
Lessons Learned
Health Canada learned that capacity to assess risk and provide a rapid response must be in place to meet the performance target to reduce the number and/or severity of health products incidents, but that these targets are heavily influenced by the unpredictability of the incidents themselves.
The Food and Nutrition program activity benefits Canadians by establishing policies, regulations and standards related to the safety and nutritional quality of food. Food safety standards are enforced by the Canadian Food Inspection Agency. The legislative framework for food is found in the Food and Drugs Act and Regulations, the Canadian Food Inspection Agency Act and the Department of Health Act. The program activity also promotes the nutritional health and well-being of Canadians by collaboratively defining, promoting and implementing evidence-based nutrition policies and standards. As the focal point and authoritative source for nutrition and healthy eating policy and promotion, the program activity disseminates timely, evidence-based and authoritative information to Canadians and stakeholders to enable them to make informed decisions and healthy choices.
| Expected Results |
Performance Indicators |
Targets | Performance Status |
Performance Summary |
|---|---|---|---|---|
|
Increased level of informed choices/healthy decisions related to food and nutrition |
Level of Stakeholder and public awareness | Over 2,000,000 requests for the 2007-2008 Canada's Food Guide, over 1,000,000 visits to the Food Guide website and over 500,000 website users creating personalized PDF files using the My Food Guide Online tool |
mostly met |
2.8 million copies of Canada's Food Guide were distributed, with 1.2 million visits to the Canada's Food Guide home page between July 2008 and June 2009. There were 500,000 views per year of the My Food Guide online tool. |
| Over 5,500 visitors using the Interactive Nutrition Labelling Quiz | exceeded | 8,177 respondents completed the Interactive Nutrition Labelling Quiz, 60% increase over 2008-2009. | ||
| Release products based on the Canadian Community Health Survey data and submit for publication articles on the nutrient intakes of children, teens, young and older adults as well as pregnant women | met all |
Health Canada continues to share and disseminate the results from the Canadian Community Health Survey 2.2, Nutrition and has produced three volumes on the usual nutrient intakes distribution from foods on a CD available through the Health Canada Online Publishing System. To support interpretation of the data tables, a series of fact sheets on the nutrient intakes of Canadian children, teens and adults has been completed and posted on the Health Canada website. A fact sheet on Aboriginal people residing off reserve has also been drafted. Health Canada also completed an article that assessed Canadian women's adherence to the 1999 gestational weight gain guidelines using data from the 2006 Maternity Experiences Survey. |
||
|
Establishment of regulatory and non-regulatory measures to address immediate areas of concern |
Number of regulatory amendments, policies and guidelines developed (as part of the Active Prevention pillar of the Food and Consumer Safety Action Plan) |
Health Canada will develop and publish: Regulatory Amendments: Enhanced Labelling for Food Allergens and Gluten Sources and Added Sulphites |
mostly met | Finalizing amendments based on comments on draft. Final publication is expected in Fall 2010. |
| Addition of Vitamins and Mineral Nutrients to Food (Food Fortification) | n/a |
A strategy change led to a review of the Health Canada food fortification policy, especially for discretionary fortification. This work is ongoing. 9 Interim Marketing Authorization (IMA) notices were published in Canada Gazette Part I. Regulatory a mendments for these 9 IMAs are expected in fiscal year 2010. |
||
| Amendments to Food Additive Tables | mostly met | 3 regulatory amendments for food additives were published in Canada Gazette Part II (13 submissions in total). Amendments were drafted for other additives. | ||
|
Policies: |
somewhat met | A revised policy was drafted for circulation to government and industry experts. | ||
| Update to Policy on Listeria monocytogenes in Ready-to-Eat Foods | met all | The draft u pdated Listeria policy was posted for comments. | ||
| Allergens update policy for precautionary statement | met all |
Current industry practices in the use of precautionary labelling surveyed and industry and public consultations were held. |
||
| Policy on Health-Related Claims about "Probiotic" Microorganisms in foods | met all |
Guidance document published. |
||
|
Guidelines: |
not met |
Delayed until 2011-2012, due to other priorities. |
||
|
Updated criteria for E. sakazakii in powdered infant formula; |
somewhat met |
Criteria drafted and external experts consulted with finalization expected in 2010-2011. |
||
|
Guidance Document for Preparing a Submission for the Authorization of Food Health Claims; |
met all |
Guidance document published. |
||
| Guidance Document -- Classification of Products at the Food-Natural Health Product Interface | met all | Guidance document published. | ||
| Number of educational tools developed (as part of the Active Prevention pillar of the Food and Consumer Safety Action Plan) |
Risk communication material on the microbial safety of fresh produce; |
met all | Guidance document published | |
| Guidance on the preparation of powdered infant formula | met all | Guidance document published | ||
|
Reduced exposure to Health Risks related to Food and Nutrition |
Proportion of Health Risk Assessments for acute health risks communicated to stakeholders within service standard | 90% within 24-48 hours (Risk 1) | exceeded | 100% |
| Proportion of Health Risk Assessments related to health risks of lesser severity communicated to stakeholders within service standards | 90% within 5-10 days (Risk 2 &3) | exceeded | 100% |
Performance Summary and Analysis
In addition to ongoing responsibilities to address food safety issues and inform Canadians about what they eat and how to handle food safely, this program activity is a key element of progress on the Food and Consumer Safety Action Plan. Resources under this program activity are allocated to continuous improvement and operation of the regulations, policies and guidelines that promote improved food safety on a daily basis and to providing information on food and nutrition for Canadians. During 2009-2010, work under this program activity led to the posting of data on transfat monitoring on the departmental website, new educational tools developed such as on allergen safety of school lunches, caffeine in food and safe handling of powdered infant formula and monitoring studies covering bottled water products, baby foods pre-packaged in glass jars and canned powered infant formula. Resources were also used or reallocated from other activities to ensure a rapid response to potential food safety risks. The need to respond immediately to those risks often means that some other commitments are delayed, as was the case for some items in 2009-2010 that show lower performance statuses in the table above.
Health Canada's food safety responsibilities were influenced by other Government commitments. As part of the Chemicals Management Plan, Health Canada analyzed priority chemicals and implemented monitoring of acrylamide to guide updated dietary exposure estimates and health risk assessments.
Lessons Learned
Health Canada develops food safety standards and policies to help minimize the risk of foodborne illnesses. The Canadian Food Inspection Agency oversees the food industry to ensure that it meets its food safety responsibilities. Health Canada has revised its 2004 Policy on Listeria monocytogenes in ready-to-eat foods. This revised policy should lead to an enhancement of the verification and control of Listeria in the food processing environment, permit earlier identification of any potential persistent contamination of the plant environment and provide an increased ability to identify and mitigate against Listeria contamination of finished products. These actions will provide an early warning and permit appropriate interventions to protect consumers.
Strategic Outcome 3 - Reduced health and environmental risks from products and substances, and healthy, systainable living and working environments
Health Canada is responsible for assessing and acting on many elements of day-to-day living that have impacts on the health of Canadians. These include drinking water safety, air quality, radiation exposure, substance use and abuse (including alcohol), consumer product safety, tobacco and second-hand smoke, workplace health, and chemicals in the workplace and in the environment. The Department is also engaged in chemical and nuclear emergency preparedness, inspection of food and potable water for the travelling public and health contingency planning for visiting dignitaries.
Much of this work is governed by legislation such as the Canadian Environmental Protection Act, 1999, the Controlled Drugs and Substances Act, the Hazardous Products Act, the Tobacco Act, the Food and Drugs Act, the Radiation Emitting Devices Act, the Quarantine Act, the Pest Control Products Act and others.
Environmental factors continue to be a key determinant of health for all Canadians. Canadians benefit from this program activity, which promotes and protects the health of Canadians by identifying, assessing and managing health risks posed by environmental factors in living, working and recreational environments. The scope of activities includes: research on drinking water quality, air quality, contaminated sites, toxicology and climate change; clean air programming and regulatory activities; risk assessment and management of: chemical substances, environmental noise, environmental electromagnetic frequencies, products of biotechnology and products of other new and emerging technologies (including nanotechnology); solar ultraviolet radiation; preparedness for radio-nuclear, chemical and biological incidents as well as working with the passenger conveyance industry to protect the travelling public.
Under the Sustainable Environmental Health program activity, Health Canada delivers on the Government of Canada's Chemicals Management Plan (CMP) by assessing the health risks of and developing risk management strategies for existing chemicals that enter the environment through manufacturing, use in consumer products, or their disposal. Key initiatives under the CMP that support this program activity include: implementing a national bio-monitoring system to track exposure to potentially harmful chemicals; working with industry sectors to develop comprehensive risk management practices that will protect Canadians and the environment; and ensuring that information about chemical substances, their hazards and practices for their safe management is available to Canadians. Under this program activity, Health Canada also works to protect the health of Canadians by assessing and managing new chemicals as well as working with other jurisdictions in improving air quality and safe drinking water.
| Expected Results |
Performance Indicators |
Targets | Performance Status |
Performance Summary |
|---|---|---|---|---|
|
Timely regulatory system response to new and emerging health risks related to chemicals or substances that are harmful to human health or the environment, and environmental risks to health. |
Proportion of regulatory activities addressed within service standards/target | To be set after baseline is established in 2011 | met all |
Screening assessment reports for Challenge and non-Challenge substances under the Chemicals Management Plan were completed and published in the Canada Gazette Part I according to the Department's timelines. Risk management instruments were developed for identified substances within expected timelines. Risk management actions imposed on 100% of new substances and products of biotechnology for which a significant risk was identified. 100% of human health risk assessments related to high priority federal contaminated sites addressed within expected timelines. |
|
New and emerging health risks related to chemicals or substances that are harmful to human health or the environment are identified, assessed and managed. |
Time period within which serious health risks are brought into a risk management regime | To be set after baseline is established in 2011 | met all |
Under the Chemicals Management Plan, risk management instruments were developed for identified substances within expected timelines. 4% of 2900 federal buildings tested for radon had rooms above the Canadian guideline for remediation. Recommendations for mitigation measures to reduce the radon levels to acceptable limits have been provided. Assessments completed for Indoor Air quality (carbon monoxide and ozone); Outdoor Air (smog and manganese); and Fuels (10% ethanol biofuel). Assessment work initiated on 7 other indoor air, outdoor air and fuel contaminants. |
|
Canadians are knowledgeable, understand and involved in environmental health issues. |
Percentage of the target population aware of environmental health issues | To be set after baseline is established in 2011 | met all |
55 stakeholder engagements across Canada , over 50% increase in web traffic and 22,000 downloads and hard copy requests for the radon guide. Over 70 media articles and interviews on radon health impacts and importance of testing and mitigation. Heat Alert and Response Systems (HARS) risk management tool developed and operational in four communities. Air Quality Health Index implementation expanded to Ottawa-Gatineau, Quebec City, Winnipeg, Saskatoon, Regina, Saint John, and St. John's and province wide in British Columbia. |
Canada's Economic Action Plan (CEAP)
Canadian Environmental Sustainability Indicators (CESI)
Research has shown that the elderly, the very young, and those with existing respiratory or cardiac conditions are particularly vulnerable to the effects of air pollution. Canadian Environmental Sustainability Indicators is a joint federal initiative with Environment Canada and Statistics Canada to support continued development of the Air Health Indicator (AHI) among others. The AHI can be determined for single or multiple locations, at a provincial, regional or national level, and for a single pollutant or for multiple pollutants concurrently. The AHI will enable refined linkages between air pollutant exposure and adverse health effects, by region, and by demographic group (e.g., age, sex), thereby helping to pinpoint the most vulnerable population groups. The AHI can be used to track changes in air pollutant levels and related health effects, both spatially and temporally, thereby helping to assess whether the most important components of the atmospheric pollutant mix were appropriately targeted for reduction.
In 2009-2010, with Canada's Economic Action Plan funding, the Department developed an AHI on Ozone, with the latest yearly data (national, regional, and by city) as well as an AHI on Fine Particulate Matter with the latest yearly data (national, regional, and by city). Health Canada also produced a Summary AHI Report as well as a report on the health impacts of exposure to Ozone and Fine Particulate Matter, including mortality due to heart, circulatory and respiratory diseases. (CEAP - Planned spending in 2009-2010: $0.3 million; Actual spending: $0.3 million.)
Performance Summary and Analysis
A major emphasis of this program activity in 2009-2010 was meeting Health Canada's responsibilities under Government of Canada environmental commitments to Canadians. From 2006 to the present, under the Chemicals Management Plan, the Department assessed the health risks of existing chemicals that enter the environment through manufacturing, use in consumer products, or their disposal, and developed risk management strategies for those chemicals where needed. Health Canada also responded to stakeholder inquiries and added to the awareness of Canadians about what they can do to reduce risks.
Recognizing the link between air quality and health, the Department continued to support the Government's Clean Air Agenda. The Air Quality Health Index is a high-profile tool that was expanded to more communities in 2009-2010, being made available in approximately 40 locations across nine provinces. Current negotiations with provincial partners may lead to further expansion across Canada.
Health Canada also expanded its work to reduce health risks from radiation/ radon in living and working environments. The Department: conducted research and published results in 29 scientific publications on the health effects of radionuclides in the
environment; assisted in improving workplace safety by providing eight quality assurance programs for the internal radiation exposure of nuclear workers and hospital/healthcare providers; reported results of more than 500,000 radiation monitoring results to Canadian workers; and ensured the protection of human health and safety
during the construction, operation and decommissioning of nuclear facilities using its Canadian radiation surveillance networks.
Health Canada identifies, assesses, manages and communicates to Canadians the health and safety risks associated with consumer products (those products that adults and children commonly use for personal, family, household and garden use or use in recreational and sports activities). The benefit of this program activity is that actions taken minimize the risks that consumer products may pose to Canadians. This is achieved through compliance and enforcement actions, consumer and industry outreach activities and surveillance and risk assessment work. Relevant acts include: Hazardous Products Act (consumer products) and Food and Drugs Act (cosmetics regulations).
| Expected Results |
Performance Indicators |
Targets | Performance Status |
Performance Summary |
|---|---|---|---|---|
|
Increase effective use of standards by industry and improved compliance with product safety obligations |
Percentage of inspected registrants/firms/users who are compliant/ non-compliant with product safety obligations |
By 2013, decreasing trend in reported product safety adverse health incidents. (Baseline to be established by 2010) |
mostly met |
Under a risk based approach, HC tests in areas where non-compliance is more likely and there is a risk. Toys - heavy metals: Toys - noise: Utility Lighters: Halloween costumes: Glazed Ceramics : Children products e.g. furniture, learning products: Children's Jewellery: |
|
Better informed consumers properly selecting and safely using products |
Number of incidents reported of improper unsafe use of consumer products |
By 2013, decreasing trend in number of reported incidents (Baseline to be established by 2010) The proposed Canada Consumer Product Safety Act and its proposed mandatory reporting of consumer product incidents, did not receive Royal Assent. As such, the baseline target identified is not attainable. The number of complaints is being used as a proxy performance indicator in the interim. |
mostly met |
Product safety complaints/incidents: 2006-07 567 complaints; 2007-2008 - 672; 2008-2009 - 944; 2009-2010 - 1102 Of the 1,102 complaints received in 2009-2010, Health Canada met its service targets, responding to 100% of complainants and met its service standard following-up with 100% of companies. Depending on the severity of the incident reported, actions included product inspection with follow-up and enforcement actions, including recall or public advisory, as appropriate, and, follow-up with the companies in question, to ensure appropriate actions have been completed. 7844 subscriptions to the Consumer Product Safety Recall website, compared with 6600 in 2008-2009. The increase in consumer reporting is linked to the increase in subscriptions to the recall website and indicates an increased consumer awareness of risks associated with consumer products. |
|
Responsive and proactive, risk-based product safety regulatory framework |
Percentage of product safety issues addressed by the new Canada Consumer Product Safety Act and its regulations | By 2013, target is 100% of issues addressed | n/a |
Not applicable in 2009-2010 as the Canada Consumer Product Safety Act has not completed the legislative approval process. |
Performance Summary and Analysis
This program activity continues to support and contribute to achieving results by ensuring that both regulated and un-regulated consumer products, cosmetics and radiation emitting devices are as safe as possible. Health Canada continues to address areas of high risk and concern through ongoing targeted inspections, surveillance and compliance promotion (both domestically and internationally) under the existing Hazardous Products Act. It also conducts outreach to Canadians on the potential dangers associated with some consumer products. For example, Health Canada issued an advisory reminding Canadians to exercise caution when using strollers with hinge mechanisms. Additionally, the Department routinely releases product recalls, for example, in a joint action with Stork Craft and the United States Consumer Product Safety Commission, Health Canada issued a drop-side crib recall affecting almost 1 million products sold in Canada.
In addition, continued market inspections on products directed for children (e.g. children's jewellery) revealed higher levels of non-compliance over the last cyclical enforcement cycle. Better surveillance techniques and increased inspection capacity led to 9 product recalls issued in the later part of the year for children's jewellery. An increasing trend in complaints/incidents received is primarily due to better information and education activities resulting in increased public knowledge. New service standards for complaint responses enabled a more rapid response to consumer complaints and issues related to consumer products.
In addition, progress against expected results is further supported by new program initiatives related to the implementation of the Food and Consumer Safety Action Plan. The cornerstone of the Action Plan is the creation of a new Canada Consumer Product Safety Act (CCPSA), which was tabled in Parliament. The introduction and passing of the proposed CCPSA and proposed new regulations and amendments to existing regulations, will provide the authority for the collection of product safety incident data from industry, through new mandatory reporting authorities. This will enable the early detection of potentially hazardous products benefitting the Canadian public and stakeholders.
Working toward the goal of reducing, preventing and enhancing the management of the risks of exposure to radiation emitting devices, we published an updated revision to Safety Code 6: Limits of Human Exposure to Radiofrequency Electromagnetic Fields, reconfirming safe exposure guidelines for radiofrequency electromagnetic energy. Efforts were also made to provide Canadians with information by publishing several It's Your Health documents on the Health Canada website, such as Airport Full Body Scanners, The Safety of Compact Fluorescent Lamps (CFLs), and Community Noise Annoyance.
Lessons Learned
A continued partnership between the United States Consumer Product Safety Commission (CPSC) and Health Canada helps to ensure that coordinated efforts and communication practices result in early identification of potentially dangerous products reaching Canadians. These relationships aid in the coordination of systems and international standards to facilitate a global approach to consumer product safety and reduce the burden on industry.
This program activity provides services to protect the health and safety of the federal public sector, visiting dignitaries, and others. Specific programs include: the provision of occupational health services to federal employees (this benefit ensures that Canada has a well-functioning and healthy public service, which, in turn, provides timely services to Canadians); delivery of the Employee Assistance Program; emergency health services to Internationally Protected Persons; and, dosimetry services (the measurement of personal, occupational exposure to radiation through the reading of "dosimeters" or plaques enclosed in special holders worn by the user for specified periods).
| Expected Results |
Performance Indicators |
Targets | Performance Status |
Performance Summary |
|---|---|---|---|---|
|
Timely system response to public service employees with psycho-social health problems |
Percentage of public service employee clients' psycho-social problems dealt with within service standards | 70% (represents the current Industry standard) |
exceeded |
95% of Public Service clients' psycho-social problems addressed within service standards; 97% satisfied with the outcome; 100% remained or returned to work. |
|
Internationally Protected Persons are protected during regular visits, major events and PM-led events from risks to their health Support to departments which enables adherence to Acts, regulations and guidelines |
Percentage of visits/events without serious health related incidents for Internationally Protected Persons (IPP) or for Canadian Public Servants | 100% | met all |
36 IPP and royal visits and 68 related health plans were developed. 98% satisfaction from lead Departments. |
Performance Summary and Analysis
The Public Service Health Program continues to transition to a new Occupational Health Medical Model which will provide efficient service delivery to client department and agencies. Surveys of the Employee Assistance Services (EAS) and Workplace Health services found extremely high satisfaction rates and reports of positive impacts on people receiving the services and on workplace issues. Trends in client satisfaction have consistently scored between 97.8 - 98.5% over the past four years.
The Internationally Protected Persons Program exceeded all its mandate requirements and objectives. There were a substantial number of high profile visits, including the Emperor of Japan, His Royal Highness, the Prince of Wales, G7 Finance Ministers meeting at Iqaluit which resulted in full health coverage and the absence of serious health incident. Strong collaboration with key stakeholders at the federal, provincial, and local levels was key to the success in meeting Health Canada commitments to internationally protected persons during the 2010 Olympic and Paralympics Games in Vancouver.
Through regulatory, programming and educational activities, Health Canada seeks to improve health outcomes by reducing and preventing tobacco consumption and addressing alcohol and drug abuse. This activity benefits Canadians by addressing the serious and adverse health effects presented by the use of tobacco products and controlled substances, which contributes to safer and healthier communities. Through the Tobacco Act and its regulations, along with the new Cracking Down on Tobacco Marketing Aimed at Youth Act, Health Canada regulates the manufacture, sale, labelling, and promotion of tobacco products. It also leads the Federal Tobacco Control Strategy - the goals of which are to: further reduce the prevalence of smoking; reduce exposure to second hand smoke; and, reduce death and disease caused by smoking.
Health Canada administers the Controlled Drugs and Substances Act and its regulations. Through four regional labs, Health Canada provides expert scientific advice and drug analysis service to law enforcement agencies. The Marihuana Medical Access Regulations control the authorization for use and cultivation of marihuana by those suffering from grave and debilitating illnesses. Health Canada is a partner in the government's National Anti-Drug Strategy which includes: prevention programming aimed at youth; facilitating access to treatment programs; compliance and enforcement activities related to controlled substances and precursor chemicals; and, increased resources to the Drug Analysis Service to support the increase in law enforcement resources.
| Expected Results |
Performance Indicators |
Targets | Performance Status |
Performance Summary |
|---|---|---|---|---|
|
The overall goal of the Tobacco Control Strategy is to reduce overall smoking prevalence from 19% (2006) to 12% by 2011 |
Smoking prevalence rate in % of the Canadian Population. | 12% (Canadian Tobacco Use Monitoring Survey) |
somewhat met |
Latest available data (2008) reported 18%. |
|
Reduced use and abuse of drugs |
Prevalence rates of drug use and abuse |
To be set after baseline is established in 2010 |
mostly met |
Latest available data (2008): Cannabis use - 11.4% (compared to 14.1% in 2004); Other illicit drug use - 12.1% (no comparable data); psychoactive pharmaceutical drug use - 28.4% (no comparable data), with 2% reporting abusing those drugs. |
|
Continued provision of high-quality evidence for law enforcement |
Number/nature of injuries and/or environmental risks caused by unsafe handling of chemicals noted by Drug Analysis Service personnel; | To be set after baseline is established in 2010 | met all | None were reported. |
| Increased compliance with legislation and regulations | Rates of compliance with policies and regulations |
To be set after baseline is established in 2010 |
met all | 84.3% tobacco retailer compliance for 2009; 85.9% for 2007-2008 and 2008-2009. |
|
Increased awareness and understanding of illicit drugs and harmful health and social effects associated with illicit drug use |
Level of awareness about harmful health and social effects associated with illicit drug use |
To be set after baseline is established in 2010 |
mostly met | 2009 National Anti-Drug Strategy Baseline Youth Survey (ages 13 to 15) showed: 1/3 had experimented with drugs; 39% said they knew a great deal about effects of drugs on physical health; 36% said they knew a great deal about effects on mental health; 48% said they would be very likely to try to stop someone close to them from using drugs; 18% have tried marijuana / cannabis at least once; 87% said cocaine is very dangerous to their health; 34% think marijuana / cannabis is very dangerous to health. |
|
Strengthened evidence-informed substance abuse treatment systems and services |
Extent to which the Drug Treatment Funding Program (DTFP) has contributed to and strengthened, evidence-informed substance abuse treatment systems and services | To be set after baseline is established in 2010 | mostly met | In early stages of implementation, demonstrated strong collaboration and commitment, e.g., increased capacity to deliver programs and services to at-risk youth through new and expanded early intervention programs and services. |
Performance Summary and Analysis
Most strategies and actions under this program activity tend to be aimed at longer-term results in reducing use of tobacco and illicit drugs. Program strategies rely on collaboration with other government departments and with provinces, territories and other stakeholders. A step forward in improving the regulatory framework controlling tobacco was Health Canada's contribution towards the passage of Bill C-32, Cracking Down on Tobacco Marketing Aimed at Youth Act, which received Royal Assent in October 2009 and will help to reduce the use of tobacco products by Canadian youth. Program results show that Health Warning Messages on tobacco product packaging are effective, and retail compliance continues to be high.
The second component of this program activity was the continued involvement in the National Anti-Drug Strategy (NADS), announced and funded in 2007. The Department provided support for community-based responses to drug issues and drug treatment services and prevention issues. The Department supports treatment programming through the Drug Treatment Funding Program (DTFP) where 13 drug treatment systems-enhancement projects and 8 treatment services projects were launched by March 31, 2010, under NADS. To support prevention programming aimed at youth, the Department continued to fund 66 projects under the Drug Strategy Community Initiatives Fund (DSCIF). Many of the DSCIF projects focus on developing prevention tools and training, to improve knowledge and skills among youth, to avoid illicit drug use.
To further support prevention programming aimed at youth, the Department contributed to the development and launch of the NADS Mass Media Campaign. This two-pronged campaign targets youth aged 13 - 15 and their parents. The parent portion of the campaign disseminated more than 45,000 NADS parent toolkits, "Talking with your Teen About Drugs." A youth mass media campaign launched in December 2009 included a 30-second TV ad driving youth to a newly created youth-friendly website: not4me.ca/0drogue.ca, which had received nearly 200,000 visits by March 31, 2010.
To help prevent unacceptable risks to people and the environment, and facilitate access to sustainable pest management tools, Health Canada, through the Pest Management Regulatory Agency, regulates the importation, sale and use of pesticides under the federal authority of the Pest Control Products Act and its Regulations.
| Expected Results |
Performance Indicators |
Targets | Performance Status |
Performance Summary |
|---|---|---|---|---|
|
Canadians have timely access to new pesticides/pesticide uses that meet standards of value, acceptable human health and environmental risk; |
Pre-market reviews and regulatory decisions on new pesticide products and new uses of pesticide products completed within performance timelines that meet international standards | 90% of reviews completed within performance timeline targets |
somewhat met |
Global Joint Reviews = 80% (5 submissions completed) |
| Only those older pesticides that meet modern standards remain registered; | Re-evaluation assessments completed within commitments under the Chemicals Management Plan | 90% of older registered pest control products have undergone a full review in the last 15 years | met all | Proposed Re-evaluation Decision documents completed for 360 of the 401 active ingredients (90%). |
| Registrants, vendors and users comply with the Pest Control Products Act and its regulations; and | Delivery of the National Pesticides Compliance Program including associated investigations / enforcement responses | 80% of compliance programs and enforcement activities delivered and reported according to timelines | met all |
Inspections = 97% (completed 615 inspections) Investigations = 86% (completed 386 investigations) Other = 903 enforcement responses |
| Canadians have access to and are using reduced risk and low risk products and risk reduction strategies. | Development of new transition strategies to use of lower risk pesticides. | Increased availability of reduced risk and low risk pesticide products | met all | Completed 2 registrations of reduced risk pesticide products. Through work with Agriculture and Agri-Food Canada, 7 reduced risk biopesticide products were registered. Facilitation of submissions and building of data packages resulted in 3 registrations and 5 submissions for low risk products. |
| Number of user groups engaged in risk reduction strategies | Increased engagement of stakeholder groups in the development of new transition strategies | mostly met | Engagement with two new stakeholder groups to develop transition strategies. |
Performance Summary and Analysis
The benefit of this program activity is to contribute to reducing health and environmental risks from pesticides and provides information to Canadians so they can make informed decisions about pesticide use. Beyond ongoing responsibilities, one major goal of this program activity has been to provide more timely access to pest control products for Canadian growers. The approach has been to work with international partners through increased use of joint reviews and work sharing. This ongoing harmonization of science and policy development continued to standardize the global approach to risk assessment processes and the management of pesticide regulation for the benefit of Canadians users of these products. The application of a risk-based approach to targeted pesticide reviews means a more efficient regulatory process.
This program activity was also influenced by the Food and Consumer Safety Action Plan during the year. Health Canada worked with manufacturers to ensure that they had systems in place to assure product integrity and to address risk situations. This included the development of best practices, in consultation with other compliance and enforcement authorities related to active prevention, targeted oversight and rapid response. Three draft documents were produced for manufacturing, distribution and disposal/recycling.
To provide Canadians with access to, and information on, reduced risk and low risk products, Health Canada worked with Agriculture and Agri-Food Canada and other stakeholders to develop and implement policies and strategies to facilitate registration of reduced risk and low risk pest control products. By adjusting the approach used, it was possible to target reviews so that evaluation efforts reflected risk levels.
Through collaboration with Environment Canada, this program activity achieved re-evaluation targets established through the Chemicals Management Plan for older pesticides products currently available on the market to determine if their continued use was acceptable in consideration of modern scientific approaches and standards.
Strategic Outcome 4 - Better health outcomes and reduction of health inequalities between First Nations and Inuit and other Canadians
Health Canada delivers or funds a range of health programs and services to First Nations and Inuit. A range of primary care services are provided in approximately 200 First Nations communities, largely in rural or remote areas where access to provincial health care services is limited. In addition, home and community care services are provided in approximately 600 First Nations communities. Health Canada supports a range of community-based health programs, focusing on children and youth, mental health and addictions, and chronic disease and injury prevention. The Department also supports a range of public health programs with a focus on communicable disease control, including tuberculosis, HIV/AIDS and vaccine-preventable diseases, environmental public health such as conducting public health inspections and monitoring drinking water quality, and research. The Non-Insured Health Benefits Program provides over 800,000 eligible First Nations and Inuit with a limited range of medically necessary health-related goods and services not provided through private insurance plans, provincial/territorial health or social programs or other publicly funded programs.
- Program Activities
- First Nations and Inuit Health Programming and Services
- Program Sub-Activities
-
- FN/I Community Programs
- FN/I Health Protection and Public Health
- FN/I Primary Care
- Non-Insured Health Benefits (supplementary) for FN/I
- Governance and Infrastructure Support to FN/I Health System
The provision of health programs and services by Health Canada to First Nations and Inuit is rooted in the Federal Indian Health Policy. The Department provides health programs and services to First Nations and Inuit as a matter of policy, using annual Appropriations Acts to obtain Parliamentary approval. Together with First Nations and Inuit and other health partners, Health Canada , through its regional offices, supports public health and community health programs on-reserve, directly benefitting First Nations and Inuit. These include environmental health and communicable and non-communicable disease prevention, and provision of primary health care services through nursing stations and community health centres in remote or isolated communities to supplement and support the services that provincial, territorial and regional health authorities provide. The Department also supports targeted health promotion programs for Aboriginal people, regardless of residency as well as counselling, addictions and mental wellness services. The Non-Insured Health Benefits coverage of drug, dental care, vision care, medical supplies and equipment, short-term crisis intervention mental health services, and medical transportation is available to all eligible First Nations and Inuit in Canada, regardless of residency.
| Expected Results |
Performance Indicators |
Targets | Performance Status |
Performance Summary |
|---|---|---|---|---|
| Better health outcomes and reduction of health inequalities between First Nations and Inuit and other Canadians | Life expectancy (at birth, on and off reserve) | N/A* | (See Note below)* | Life expectancy (at birth, on and off reserve): Canada - Overall - 79.6 - Males - 77.0 - Females - 82.0 Registered Indians - Overall - 72.9 (gap - 6.7 yrs) - Males - 70.4 (gap - 6.6 yrs) - Females - 75.5 (gap - 6.5 yrs) Inuit Regions - Overall - 66.9 (gap - 12.7 yrs) - Males - 64.4 (gap - 12.6 yrs) - Females - 69.8 (gap - 12.2 yrs) |
| Birth weight | Canada (2002-2003) - 6.0% (low), 13% (high) First Nations on-reserve (2002-2003) - 5.5% (low), 21% (high) Inuit-inhabited areas (1990-2000) - 6.7% (low), 13.1% (high) |
|||
| Mortality | Overall mortality for First Nations (2000) is 1.4x higher than for the Canadian population (1999) | |||
| Diabetes Rates | 2002/03 Canada - 5.2% First Nations on-reserve - 19.7% (3.8x higher) 2005/06 Canada - 5.1% Inuit Nunangat - 3% (41% lower) |
|||
| Suicide Rates | The rate of First Nations youth suicide (10 to 19 years) was 4.3 times greater than for Canada in 2000. Suicide rate for Inuit regions (1999-2003) is 11.6 times higher than for the rest of Canada. |
|||
| Incidence of Tuberculosis | Rate per 100,000 pop. For 2007 Canada - 4.7 Registered Indians - 27.9 (5.9x higher) Inuit Regions - 84.2 (17.9 times higher) |
|||
| Non-Insured Health Benefit (NIHB) Client utilization rates | For 2009-2010, the national utilization rate for pharmacy benefit was 64%. Regional rates ranged from 73% in Saskatchewan to 46% in Nunavut. |
*Note: Health Canada continues to work with its federal (e.g. Statistics Canada, Indian and Northern Affairs Canada) provincial and territorial partners as well as with First Nations and Inuit to improve the quality and accessibility of performance indicator data. Many indicators (e.g. life expectancy, mortality) only show changes over the very long-term.
Canada's Economic Action Plan (CEAP)
Strengthened Non-Insured Health Benefits Program and enhanced support for primary care services for First Nations and Inuit
Budget 2009 included $102.4 million for 2009-2010 to strengthen the Non-Insured Health Benefits Program for First Nations and Inuit. The Non-Insured Health Benefits Program (NIHB) provides approximately 830,000 eligible First Nations and Inuit with a limited range of medically necessary health-related goods and services not provided through private insurance plans, provincial/territorial health or social programs, or other publicly-funded programs. These include prescription drug benefits, dental benefits, vision care benefits, medical supplies and equipment benefits, medical transportation, short-term, mental health crisis intervention counselling, and provincial health premiums in British Columbia.
Budget 2009 also included $32.4 million for 2009-2010 to enhance support for primary care nursing services for First Nations. Expected results from CEAP funding include the continuation of primary care nursing in remote and isolated First Nations communities on a 24 hour, 7 day per week basis; and, stabilizing the First Nations and Inuit health system in order to improve health services for First Nations and better align federal and provincial service standards.
CEAP panned spending in 2009-2010: $134.5 million. Actual spending: $134.5 million.
Health Facilities and Capital for First Nations and Inuit
To ensure that First Nations continue to have access to safe and effective facilities which house needed health programs and services, CEAP funded new construction and renovation projects for health services infrastructure benefiting First Nations, including health centres and nurses' residences. A total of 40 new major construction projects and approximately 230 minor renovation projects will be completed by March 31, 2011. Projects have undergone a rigorous program planning phase that included developing all pre-construction architectural, engineering and design work. These measures ensured that most projects could commence immediately following approval of funds.
As of March 31, 2010, 40 contribution agreements had been signed for major capital projects of which one has already completed construction, 23 are at the construction stage, eight are out to tender, with the remaining projects at the design stage. Numerous renovation projects to existing health facilities infrastructure are also advancing in First Nations communities.
CEAP planned spending in 2009-2010: $67.4 million. Actual spending: 67.4 million
The following link shows the new projects, their project value and anticipated completion dates: http://www.hc-sc.gc.ca/ahc-asc/media/nr-cp/_2009/2009_143bk2-eng.php
Performance Summary and Analysis
As the sole program activity in a strategic outcome that encompasses the majority of Health Canada spending, a variety of strategies are in place to guide the use of resources for ongoing responsibilities and to meet targeted health priorities. Operationally, Health Canada maintained standards of care for First Nations and Inuit health programs and services. Funds provided from Canada's Economic Action Plan enabled stabilization of key services as noted above.
Another element of this program activity was the variety of individual initiatives and programs that address specific Aboriginal health challenges. The Department used evaluations, studies, consultations, surveys and other approaches to assess the Aboriginal Diabetes Initiative, the Maternal Child Health Program, the National Aboriginal Youth Suicide Prevention Strategy, and other programs. The evidence is being used to shape ongoing improvements to these initiatives, many of which received renewed funding through Budget 2010 announcements. Health Canada continued to move forward in modernizing addictions services by increasing their accessibility, quality and effectiveness. Eight multidisciplinary, community-based Mental Wellness Teams Pilots are in various stages of implementation, with one being fully operational.
In response to the H1N1 influenza pandemic, Health Canada worked with First Nations communities to complete pandemic plans, reallocate health human resources as needed, and collaborate with all levels of government. This experience highlighted the need to maintain enough flexibility in programs and services. Having this flexibility allowed the Department to realign priorities and resources to respond to this event.
Many priorities under this program activity are linked to broader Government of Canada commitments and investments. A good example is the development of a National Wastewater Framework as part of the National Framework for the Environmental Public Health Program in First Nations Communities South of 60 Degrees. Health Canada has increased drinking water sampling and testing for quality at the tap in order to protect public health. As a more fundamental longer-term goal, Health Canada supported efforts with Indian and Northern Affairs Canada to engage First Nations toward the development of a legislative framework for drinking water and wastewater in First Nations communities that would be adapted based on existing provincial and territorial regulations.
Facilitating a more efficient, effective and accountable health system for First Nations and Inuit, continued to be an important strategic direction. The Aboriginal Health Transition Fund (AHTF), improved integration and adaptation of existing health services through the development of multi-partner joint service protocols, referral/discharge and information systems, collaborative committees, and governance structures and/or processes that better link dedicated health services for First Nations and Inuit with other health services and systems. This work included tripartite discussions and health system alignment processes. For example, Health Canada, the Government of British Columbia and the British Columbia First Nations Leadership Council continue to work toward implementation of the commitments made in the 2007 Tripartite First Nations Health Plan.
The overall approach to improving Aboriginal health also envisions greater participation by Aboriginal people in health careers. A key to this was completion of the initial five-year mandate of the Aboriginal Health Human Resources Initiative with results that were well above targets. In 2009-2010, 507 bursaries and scholarships were awarded to First Nations and Inuit health career students, while 90 post-secondary projects were implemented including student support programs, bridging and access programs, and support for curriculum adaptation and / or improved cultural competency for future health care providers. Health Canada continued efforts to recruit and retain nurses who work in remote and isolated First Nations communities.
Lessons Learned
Lessons learned in the past year include the importance of allocating sufficient time and resources for constructive consultations with multiple stakeholders, and the challenges of realigning priorities and resources to respond to unexpected events such as H1N1 influenza pandemic.
Canada's Economic Action Plan (CEAP)
Maintenance and modernization of Health Canada Laboratories
Health Canada is investing $16.3 M over two years in its custodial role in four of its laboratories to address building code, fire/life safety, barrier-free accessibility issues, and compliance with regulations as well as addressing deferred maintenance and recapitalization of assets. Five individual projects are on schedule and14 projects have been completed. (CEAP Planned spending in 2009-2010, $9.0 M, Actual spending $9.0 M.)
Funding of $0.7 M for Arctic research facilities was transferred from INAC to Health Canada in 2009-2010, and is included in Health Canada's CEAP spending.
Performance Summary and Analysis
In addition to performance linked to departmental priorities and strategic outcomes, Health Canada is supported by ongoing Internal Services activities and initiatives. Performance Highlights for the 2009 / 2010 fiscal year include:
H1N1 - Significant time and resources were directed toward the H1N1 response. A Departmental Coordinating Committee was formed to ensure effective communications, coordination of actions and the delivery of results. A Real-Time Absenteeism Tracking Tool was developed to support the Department's efforts in anticipating potential workforce shortages, and securing or reallocating resources had there been an escalation in the H1N1 pandemic. Communications initiatives were also heightened with the development of managers' guides and enhanced communications and employee updates related to H1N1.
Governance and Management Support:
Integrated Planning - The Department further integrated its business planning with financial, human resources, IT, investment and facilities management planning processes. This improved integration resulted in the development of an annual Departmental Operational Plan (DOP) outlining the initiatives and activities to be undertaken for the year to come. Exceeding requirements articulated in the Clerk of the Privy Council's Action Plan, the DOP was used to communicate to employees expected activities and deliverables, and served as a vehicle to identify accountabilities.
Science Plan and Science-Policy Interface - A Health Canada Science Plan has been developed, aimed at establishing science priorities over the next 3-5 years, improving the management of science within the Department and strengthening the links between science and decision making. Based on extensive consultations both internal and external to the Department, (an Interdepartmental Science Policy Interface Workshop on best practices was held Sept 2009 and the First Health Canada Science Policy Roundtable was held in November) department-wide science needs have been identified to establish science priorities, as well as priorities for policy work and related evidence gathering and analysis over the longer term. Centers of Expertise have been established in 4 areas: nanotechnology, risk assessment, bioethics, and S&T foresight.
The Science Excellence Framework and a Nanotechnology policy approach and workplan were developed. Five Roundtables/ Workshops were held: Interdepartmental Science Policy Interface Workshop on best practices; the First Health Canada Science Policy Roundtable; the Health Portfolio Evidence-Based Workshop; a joint HC/CIHR Best Brains Exchange; and an Inquiry on Strengthening the Science Policy Interface. Work is proceeding on the renewal of the laboratory infrastructure and revitalizing the non-lab infrastructure, including the completion of an Options and Costing Analysis and consultations, and data analysis of laboratory status/needs.
Resource Management Services:
Human Resources - The Talent Management Strategy is intended to maximize investment in people at all levels and in all areas of expertise. This ongoing priority for the Department is on schedule overall, in spite of initial delays due to competing priorities related to supporting the H1N1 response, budget reductions, and capacity issues. Two initiatives under the strategy were dropped at mid-year (proposal for 1-800 My Career and Expansion of TM questionnaire to non Executive levels). Consolidation of Learning Centres/ facilities was completed in April, 2010, resulting in a cost saving of $1M.
New collective staffing strategies were implemented. This has streamlined the staffing process, reduced duplication of efforts, and has served as an effective tool for hiring managers. This past year, collective staffing appointments accounted for 52.5% of entry mid-level Administrative actions, exceeding the Department's own target. PeopleSoft will replace the current outdated HR IM system in order to improve enterprise information, enhance services to support program delivery, streamline processes and reduce cost. The Department has moved forward in establishing a governance structure, developed business requirements and a full project plan. Implementation will begin in the new fiscal year.
IM/IT- Health Canada (HC), in partnership with PWGSC IT Shared Services, is the first federal department to adopt a new innovative interoperable Web 2.0 tool called Oracle Beehive. The Business Enterprise Enabler (BEE) initiative provides Health Canada users with access to collaboration tools such as wiki's and blogs, team workspaces and instant messaging. This will enable HC to use industry leading services for enterprise collaboration, while aligning with the Government of Canada IT Shared Services initiative. Health Canada will continue to roll-out Web 2.0 tools, in response the Clerk's directions regarding increased use of wikis and blogs in government.
Finance and Internal Controls - The Department incorporated a series of measures to equip its staff to manage financial risks, by: raising awareness; providing appropriate knowledge and tools; training and development in financial management; and, by documenting main business processes and key risk and control points to support the management and oversight of its control systems. Consistent and standardized financial management processes were put into place, new processes for standardized salary costs and forecasts, and financial coding, have been completed and implemented . Over the past year, the Department has completed the documentation of key business processes and related internal controls over financial reporting. This work was required as part of the departmental Readiness Assessment Action Plan developed to assist with the preparation of future auditable Financial Statements. The Department is now moving towards monitoring the effectiveness of these internal controls.
Asset Management Services:
Real Property - The Department has achieved a total of $6M in savings through the Real Property Modernization Initiative allowing HC to increase efficiencies, improve services to HC clients, and provide better value for money for taxpayers. The efficient use of space credits totalled a savings of $1.8M, exceeding the original cost reduction target by $700K; the development of new MOUs generated a total saving of $236K; the repatriation of the client service function from PWGSC resulted in an additional $1M annual cost savings; and implementation of a multi-year plan to reduce HC reimbursing lease costs realized an annual ongoing savings of $3M. The Real Property (RP) Framework has been developed and approved in accordance with the road map. Progress on the remaining two elements, the RP Integrated Risk and Performance Management Framework and the RP Integrated Information Management Framework, is on schedule.
Section III - Supplementary Information
Financial Highlights
| Condensed Statement of Financial Position At end of Fiscal Year (March 31, 2010) |
% Change |
2008-09 | 2009-10 |
|---|---|---|---|
| Assets | -17% | 636,410 | 530,507 |
| Total Assets | -17% | 636,410 | 530,507 |
| Total | -17% | $636,410 | $530,507 |
| Liabilities | 33% | 969,750 | 1,256,282 |
| Total Liabilities | 33% | 969,750 | 1,256,282 |
| Equity | 127% | -333,340 | -725,775 |
| Total Equity | 127% | -333,340 | -725,775 |
| Total | -17% | $636,410 | $530,507 |
| Condensed Statement of Operations At end of Fiscal Year (March 31, 2010) |
% Change |
2008-09 | 2009-10 |
|---|---|---|---|
| Expenses | 20% | 3,607,649 | 4,306,900 |
| Total Expenses | 20% | 3,607,649 | 4,306,900 |
| Revenues | 0% | 84,839 | 84,969 |
| Total Revenues | 0% | 84,839 | 84,969 |
| Net Cost of Operations | 20% | $3,522,810 | $4,221,931 |
Refer to the full Statement of Management Responsibility for further details
http://www.hc-sc.gc.ca/ahc-asc/performance/estim-previs/dpr-rmr/2009-2010-smr-drd-eng.php
Assets by Type
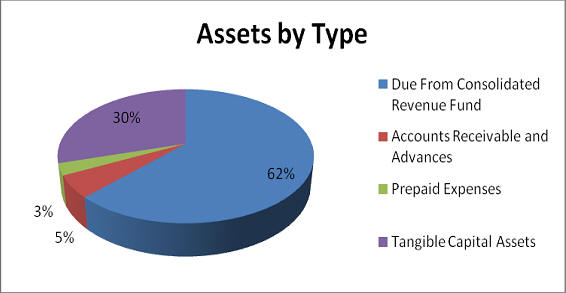
Total assets were $530.5M at the end of 2009-10, a decrease of $105.9M over the previous year. The majority of the change was due to a decrease in Due From the Consolidated Revenue Fund account of $132.8M, offset by increases in Capital Assets $17.8M, Accounts Receivable and Advances $5.3M and Prepaid Expenses $3.8M
Liabilities by Type
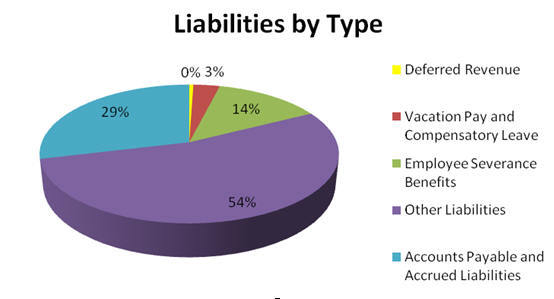
Total liabilities were $1,256.3M at the end of 2009-10, an increase of $286.5M over the previous year. $432.8M of the net increase in liability is a result of $500.0M provided for Canada Health Infoway Inc. from Budget 2009 less a payment of $67.2M from the liability to the same organization for Budget 2007. This increase was partially offset by net reductions to employee severance benefits and accounts payable and accrued liabilities.
Expenses by Strategic Outcome
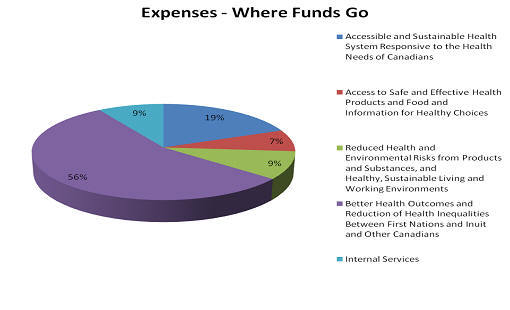
The department's total expenses were $4.3B in 2009-10, an increase of $699.3M over 2008-09. This was due mainly to increases in Transfer Payments ($653.2M), Salaries and Wages ($21.5M) and travel for non-insured health patients ($15.5M).
Revenues by Strategic Outcome
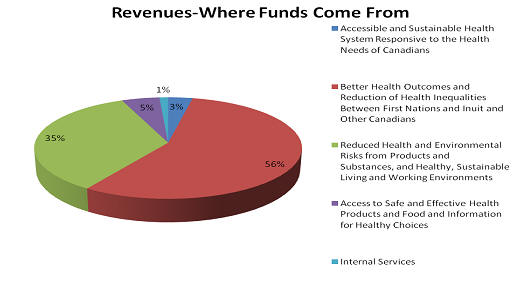
Health Canada receives most of its funding through annual Parliamentary appropriations. The department uses the Consolidated Revenue Fund (CRF) which is administered by the Receiver General for Canada. All cash received is deposited to the CRF and all cash disbursements are paid from the CRF. Health Canada does however generate revenue from program activities that support the above-noted Strategic Outcomes. The department's total revenue was $85.0M in 2009-10, an increase of $130.0K over 2008-09.
Financial Statements
2009-2010 Statement of Management Responsibility
Supplementary Information Tables
All electronic supplementary information tables for the 2009-2010 Departmental Performance Report can be found on the Treasury Board of Canada Secretariat's website at: http://tbs-sct.gc.ca/dpr-rmr/st-ts-eng.asp.
- Details on Transfer Payment Programs (TPPs)
- Green Procurement
- Horizontal Initiatives
- Internal Audits and Evaluations
- Response to Parliamentary Committees and External Audits
- Sources of Respendable and Non-Respendable Revenue
- Status Report on Major Crown/Transformational Projects
- Up-Front Multi-Year Funding
- User Fees Reporting
Web Links
- Aboriginal Health Human Resources Initiative
http://www.hc-sc.gc.ca/ahc-asc/activit/strateg/ahhri-irrhs-eng.php - Aboriginal Health Needs
http://www.afmc.ca/social-aboriginal-health-e.php - Aboriginal Health Transition Fund
http://www.hc-sc.gc.ca/fniah-spnia/services/acces/adapt-env-eng.php - Air Quality
http://www.ec.gc.ca/Air/default.asp?lang=En&n=04104DB7-1 - Air Quality Health Index
http://www.ec.gc.ca/cas-aqhi/default.asp?Lang=En - Airport Full Body Scanners
http://www.hc-sc.gc.ca/hl-vs/iyh-vsv/life-vie/airport-scanners-aeroports-eng.php - Asia-Pacific Economic Cooperation
http://www.apec.org - Assisted Human Reproduction Act
http://laws.justice.gc.ca/en/A-13.4/ - Assisted Human Reproduction Canada
http://www.ahrc-pac.gc.ca/ - Canada Consumer Product Safety Act
http://www.hc-sc.gc.ca/cps-spc/legislation/acts-lois/ccpsa-lcspc/index-eng.php - Canada's Economic Action Plan
http://www.actionplan.gc.ca/eng/index.asp - Canada's Food Guide
http://www.hc-sc.gc.ca/fn-an/food-guide-aliment/index-eng.php - Canada Health Act
http://www.hc-sc.gc.ca/hcs-sss/medi-assur/cha-lcs/index-eng.php - Canada Health Infoway
http://www.infoway-inforoute.ca/ - Canadian Community Health Survey
http://www.statcan.gc.ca/cgi-bin/imdb/p2SV.pl?Function=getSurvey&SDDS=3226&lang=en&db=imdb&adm=8&dis=2 - Canadian Environmental Protection Act
http://laws.justice.gc.ca/en/C-15.31/ - Canadian Environmental Sustainability Indicators
http://www.statcan.gc.ca/pub/16-251-x/16-251-x2005000-eng.htm - Canadian Food Inspection Agency
http://www.inspection.gc.ca/english/toce.shtml - Canadian Food Inspection Agency Act
http://laws.justice.gc.ca/en/C-16.5/ - Canadian Institute for Health Information
http://secure.cihi.ca/cihiweb/dispPage.jsp?cw_page=home_e - Canadian Radiological Monitoring Network
http://www.hc-sc.gc.ca/ewh-semt/contaminants/radiation/crmn-rcsr/index-eng.php - Canadian Tobacco Use Monitoring Survey
http://www.statcan.gc.ca/dli-ild/data-donnees/ftp/survey-tobacco-enquete-tabac-eng.htm - Chemicals Management Plan
http://www.chemicalsubstanceschimiques.gc.ca/plan/index_e.html - Chemical Substances
http://www.chemicalsubstanceschimiques.gc.ca/index-eng.php - Clean Air Agenda
http://www.sct.gc.ca/hidb-bdih/initiative-eng.aspx?Org=0&Hi=12 - Clean Air Regulatory Agenda
http://www.hc-sc.gc.ca/ewh-semt/air/regulatory-reglementation-eng.php - Community Noise Annoyance
http://www.hc-sc.gc.ca/hl-vs/iyh-vsv/life-vie/community-urbain-eng.php - Consumer Product Recalls
http://cpsr-rspc.hc-sc.gc.ca/PR-RP/home-accueil-eng.jsp - Consumer Product Safety
http://www.hc-sc.gc.ca/cps-spc/index-eng.php - Consumer Product Safety Commission
http://www.cpsc.gov/ - Consumer Safety Portal
http://www.hc-sc.gc.ca/cips-icsp/index-eng.php - Controlled Drugs and Substances Act
http://laws.justice.gc.ca/en/C-38.8/ - Controlled Substances
http://www.hc-sc.gc.ca/hc-ps/substancontrol/substan/index-eng.php - Cracking Down on Tobacco Marketing Aimed at Youth Act
http://www2.parl.gc.ca/Sites/LOP/LegislativeSummaries/Bills_ls.asp?lang=E&ls=c32&source=library_prb&Parl=40&Ses=2 - Department of Health Act
http://laws.justice.gc.ca/en/H-3.2/index.html - Drinking Water and Wastewater
http://www.hc-sc.gc.ca/fniah-spnia/promotion/public-publique/water-eau-eng.php - Drug Analysis Service
http://www.hc-sc.gc.ca/hc-ps/substancontrol/analys-drugs-drogues/index-eng.php - Drug Product Database
http://www.hc-sc.gc.ca/dhp-mps/prodpharma/databasdon/index-eng.php - Drug Safety and Effectiveness Network (DSEN)
http://www.cihr-irsc.gc.ca/e/40269.html - Drug Strategy Community Initiatives Fund
http://www.hc-sc.gc.ca/hc-ps/drugs-drogues/dscif-ficsa/index-eng.php - Drug Treatment Funding Program
http://www.hc-sc.gc.ca/ahc-asc/media/nr-cp/_2008/2008_64bk-eng.php - Emergency Preparedness
http://www.hc-sc.gc.ca/hc-ps/ed-ud/prepar/index-eng.php - Federal Indian Health Policy
http://www.hc-sc.gc.ca/ahc-asc/branch-dirgen/fnihb-dgspni/poli_1979-eng.php - Federal Tobacco Control Strategy
http://www.hc-sc.gc.ca/hc-ps/tobac-tabac/about-apropos/role/federal/strateg-eng.php - First Nations Health Managers Competency Framework (PDF version)
http://www.fnhealthmanagers.ca/docs/e/FNHM_Comp_Framework-English.pdf - Food and Consumer Safety Action Plan
http://www.tbs-sct.gc.ca/hidb-bdih/initiative-eng.aspx?Hi=85 - Food and Drugs Act
http://laws.justice.gc.ca/en/F-27/ - Food and Nutrition
http://www.hc-sc.gc.ca/fn-an/index-eng.php - Hazardous Products Act
http://laws.justice.gc.ca/en/H-3/ - Health Canada Food Fortification Policy
http://www.hc-sc.gc.ca/fn-an/nutrition/vitamin/fortification_factsheet2-fiche2-eng.php - Health Canada Science Forum
http://www.hc-sc.gc.ca/sr-sr/about-apropos/promotion/index-eng.php - Health Canada Science Plan
http://www.consultations.hc-sc.gc.ca/public-consult/consultations/calendar-calendrier/consultation_e.php?id=299 - Health Care System
http://www.hc-sc.gc.ca/hcs-sss/index-eng.php - Health Concerns
http://www.hc-sc.gc.ca/hc-ps/tobac-tabac/index-eng.php - Health Human Resource Strategy
http://www.hc-sc.gc.ca/hcs-sss/hhr-rhs/strateg/index-eng.php - Health Policy Research Bulletin
http://www.hc-sc.gc.ca/sr-sr/pubs/index-eng.php - Healthy Canada: A federal report on comparable health indicators, 2008 (PDF version)
http://www.hc-sc.gc.ca/hcs-sss/alt_formats/hpb-dgps/pdf/pubs/system-regime/2008-fed-comp-indicat/index-eng.pdf - Internationally Educated Health Professionals Initiative
http://www.hc-sc.gc.ca/hcs-sss/finance/hcpcp-pcpss/iehpi-ipsfe-eng.php - It's Your Health
http://www.hc-sc.gc.ca/hl-vs/iyh-vsv/index-eng.php - Listeria
http://www.hc-sc.gc.ca/fn-an/consultation/init/_listeria/draft-ebauche-eng.php - Marihuana Medical Access Regulations
http://www.hc-sc.gc.ca/dhp-mps/marihuana/index-eng.php - MedEffect Canada
http://hc-sc.gc.ca/dhp-mps/medeff/index-eng.php - Medical Devices
http://www.hc-sc.gc.ca/dhp-mps/md-im/index-eng.php - National Aboriginal Achievement Foundation
http://www.naaf.ca - National Anti-Drug Strategy
http://www.nationalantidrugstrategy.gc.ca/ - National Calibration Reference Centre
http://www.hc-sc.gc.ca/ewh-semt/occup-travail/radiation/invivo/index-eng.php - National Dose Registry
http://www.hc-sc.gc.ca/ewh-semt/occup-travail/radiation/regist/index-eng.php - National Dosimetry Services
http://hc-sc.gc.ca/ewh-semt/occup-travail/radiation/dosim/index-eng.php - Natural Health Product
http://www.hc-sc.gc.ca/dhp-mps/prodnatur/index-eng.php - Natural Health Product Interface
http://www.hc-sc.gc.ca/dhp-mps/prodnatur/legislation/docs/food-nhp-aliments-psn-guide-eng.php - Non-Insured Health Benefits
http://www.hc-sc.gc.ca/fniah-spnia/nihb-ssna/index-eng.php - Official Language Health Contribution Program
http://www.hc-sc.gc.ca/ahc-asc/branch-dirgen/rapb-dgrp/pd-dp/olcdb-baclo-eng.php - Official Language Minority Communities
http://www.hc-sc.gc.ca/ahc-asc/branch-dirgen/rapb-dgrp/pd-dp/olcdb-baclo-eng.php - Pan American Health Organization
http://new.paho.org/hq/ - Patient Wait Time Guarantee
http://www.hc-sc.gc.ca/hcs-sss/finance/hcpcp-pcpss/pwgt-gtap-eng.php - Permit the use of caffeine and caffeine citrate
http://gazette.gc.ca/rp-pr/p1/2010/2010-03-20/html/notice-avis-eng.html#d106 - Permit the use of carrageenan and tocopherols
http://gazette.gc.ca/rp-pr/p1/2009/2009-07-11/html/notice-avis-eng.html#d111 - Permit the use of lecithin
http://gazette.gc.ca/rp-pr/p1/2009/2009-07-18/html/notice-avis-eng.html#d101 - Permit the use of sodium copper chlorophyllin
http://gazette.gc.ca/rp-pr/p1/2009/2009-08-08/html/notice-avis-eng.html#d109 - Permit the use of sodium tripolyphosphate
http://gazette.gc.ca/rp-pr/p1/2009/2009-11-07/html/notice-avis-eng.html#d118 - Permit the use of sucralose
http://gazette.gc.ca/rp-pr/p1/2009/2009-06-13/html/notice-avis-eng.html#d117 - Permit the use of the enzyme amylase
http://gazette.gc.ca/rp-pr/p1/2010/2010-03-06/html/notice-avis-eng.html#d108 - Permit the use of the phospholipase A 2 enzyme
http://gazette.gc.ca/rp-pr/p1/2009/2009-2010-10/html/notice-avis-eng.html#d117 - Permit the use of the xylanase enzyme
http://gazette.gc.ca/rp-pr/p1/2009/2009-08-08/html/notice-avis-eng.html#d108 - Pest Control Products Act
http://laws.justice.gc.ca/en/P-9/index.html - Pest Management Regulatory Agency
http://www.hc-sc.gc.ca/ahc-asc/branch-dirgen/pmra-arla/index-eng.php - Powdered Infant Formula
http://www.hc-sc.gc.ca/fn-an/nutrition/child-enfant/infant-nourisson/pif-ppn-recommandations-eng.php - Precautionary Labelling of Food Allergens
http://www.hc-sc.gc.ca/fn-an/consultation/_allergen2009/index-eng.php - Preparing a Submission for Food Health Claims
http://www.hc-sc.gc.ca/fn-an/legislation/guide-ld/health-claims_guidance-orientation_allegations-sante-eng.php - Produce Safety
http://www.hc-sc.gc.ca/fn-an/securit/kitchen-cuisine/safety-salubrite/index-eng.php - Public Health Agency of Canada
http://www.phac-aspc.gc.ca/index-eng.php - Quarantine Act
http://laws.justice.gc.ca/en/Q-1/ - Radiation
http://www.hc-sc.gc.ca/ewh-semt/radiation/index-eng.php - Radiation Emitting Devices Act
http://laws.justice.gc.ca/en/R-1/index.html - Radiofrequency Exposure Guidelines
http://www.hc-sc.gc.ca/ewh-semt/pubs/radiation/radio_guide-lignes_direct-eng.php - Radiological Impact
http://www.hc-sc.gc.ca/ewh-semt/contaminants/radiation/impact/index-eng.php - Radon
http://www.hc-sc.gc.ca/ewh-semt/radiation/radon/index-eng.php - Safety of Compact Fluorescent Lamps
http://www.hc-sc.gc.ca/hl-vs/iyh-vsv/prod/cfl-afc-eng.php - Safety Procedures for the Installation, Use and Control of X-ray Equipment in Large Medical Radiological Facilities
http://www.hc-sc.gc.ca/ewh-semt/pubs/radiation/safety-code_35-securite/index-eng.php - Strengthening Aboriginal Health Human Resources
http://casn.ca/en/Making_it_Happen_:_Strengthening_Aboriginal_Health_Human_Resources_118/items/Links_6.html - Tobacco Act
http://laws.justice.gc.ca/en/T-11.5/ - Tripartite First Nations Health Plan
http://www.hc-sc.gc.ca/fniah-spnia/pubs/services/2007-06_tripartite_plan/index-eng.php - Use of Probiotic Microorganisms in Food
http://www.hc-sc.gc.ca/fn-an/legislation/guide-ld/probiotics_guidance-orientation_probiotiques-eng.php - Water Quality
http://www.hc-sc.gc.ca/ewh-semt/water-eau/index-eng.php - World Health Organization
http://www.who.int/en/