
Treasury Board of Canada Secretariat
www.tbs-sct.gc.ca
Common menu bar links
Breadcrumb Trail
ARCHIVED - Canadian Institutes of Health Research - Report
 This page has been archived.
This page has been archived.
Archived Content
Information identified as archived on the Web is for reference, research or recordkeeping purposes. It has not been altered or updated after the date of archiving. Web pages that are archived on the Web are not subject to the Government of Canada Web Standards. As per the Communications Policy of the Government of Canada, you can request alternate formats on the "Contact Us" page.
Minister's Message
I am pleased to present the 2009-2010 Departmental Performance Report (DPR) for the Canadian Institutes of Health Research (CIHR).
The Government of Canada is committed, through our Science and Technology Strategy, to supporting cutting-edge research in areas of Canadian strength, including health research. CIHR is a critical component in our efforts to find solutions to some of our most pressing health issues, and in our efforts to move innovations from research into our health system and into the marketplace.
Through its funded research, CIHR is building the knowledge base that allows us to meet the challenge of ensuring the health and well-being of Canadians. Through its commitment to knowledge translation, CIHR is ensuring that the knowledge created through its funded research is applied in the form of new products, services and health care practices; improvements to policies and programs; and new tools used to help individuals maintain and enhance their own health.
This has been an eventful year for CIHR. Last fall, CIHR launched Health Research Roadmap: Creating innovative research for better health and health care, a five-year strategic plan that will take CIHR to 2013-14. Roadmap builds on CIHR's successes to date and sets out four strategic directions: invest in world-class research excellence; address health and health system research priorities; accelerate the capture of health and economic benefits of health research; and achieve organizational excellence, foster ethics and demonstrate impact.
Already, CIHR is at work on efforts to implement its new strategic directions. As an example, it has launched a national discussion on the important topic of patient-oriented research. During the past year, CIHR held consultations with governments, industry, health charities, academic healthcare organizations and other stakeholders to determine priorities for a patient-oriented research strategy and the steps required to implement such an initiative.
CIHR played a critical role in the Government of Canada's response to the H1N1 outbreak and the medical isotope shortage, in both cases investing in rapid response research to provide the evidence the Government of Canada needed to support action and make decisions for the future in both of these important areas. CIHR has also looked ahead to future health-care challenges, such as the growing numbers of Canadians suffering from Alzheimer's disease. In response, CIHR created an International Collaborative Research Strategy for Alzheimer 's disease. A France-Quebec-Canada joint funding initiative for Alzheimer's disease was launched in September 2009 and collaborations with the UK and Germany are in development.
As the above examples highlight, CIHR has excelled in its efforts to build partnerships with universities, academic healthcare organizations, charitable organizations, industry and international partners to maximize the impact of federal investment in health research, and to support excellence among Canada's best and brightest health researchers. CIHR's initiatives underscore its commitment to promoting excellence in health research for the benefit of all Canadians, now and in the future.
The Honourable Leona Aglukkaq, P.C., M.P.
Minister of Health
Government of Canada
Section I – Departmental Overview
Raison d’�tre & Responsibilities
CIHR is the Government of Canada's premier health research funding agency. It was created in June 2000 by the CIHR Act with a mandate "to excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health care system".
CIHR responds to the evolving needs of health research by:
- Supporting outstanding research, both investigator-driven and strategic (i.e. targeted on priority areas), across all health sectors;
- Building research capacity by supporting researchers in under-developed areas and training the next generation of health researchers; and
- Promoting knowledge translation, so that the results of research are transformed into relevant applications (policies, practices, procedures, products and services), that have health and economic benefits.
At CIHR's inception, 13 institutes were created. These institutes are not "bricks-and-mortar" buildings but communities of experts. In its topic area, each of CIHR's 13 Institutes supports a broad spectrum of research: biomedical, clinical, health services and systems, and population and public health. Institutes form national research networks linking researchers, funders and knowledge users across Canada to work on priority areas. This innovative structure has been hailed as a global best practice and supports a solution-focused, multidisciplinary and collaborative approach to health research.
CIHR is governed by a Governing Council of 16 members. The President of CIHR serves as its Chair, with the Deputy Minister of Health an ex-officio and non-voting member. CIHR reports to Parliament through the Minister of Health and, as such, plays a key role in the Health Portfolio.
CIHR works closely with Natural Sciences and Engineering Research Council (NSERC) and Social Sciences and Humanities Research Council (SSHRC) to share information and co-ordinate research efforts. The three Councils collectively manage several flagship programs for the Government of Canada, including the Networks of Centres of Excellence Program, the Canada Graduate Scholarships Program, the Vanier Graduate Scholarship Program, and the Canada Research Chairs Program. In 2010-11, CIHR will introduce the Banting Post-doctoral Fellowships Program.
In 2009-10, CIHR continued to support the Government of Canada's Science & Technology Strategy. CIHR's focus on excellence and innovation helps ensure that its investments are aligned to the Strategy's key theme of mobilizing S&T to Canada's advantage.
CIHR Quick facts: 2009-2010
President: Dr. Alain Beaudet, MD, PhD
Annual Spending: $983.7 Million
Head Office: Ottawa
Employees: 396
Institutes: 13
Aboriginal Peoples' Health: Dr. Malcolm King
Aging: Dr. Anne Martin-Matthews
Cancer Research: Dr. Morag Park
Circulatory and Respiratory Health: Dr. Peter Liu
Gender and Health: Dr. Joy Johnson
Genetics: Dr. Roderick McInnes
Health Services and Policy Research: Dr. Colleen M. Flood
Human Development, Child and Youth Health: Dr. Michael Kramer
Infection and Immunity: Dr. Marc Ouellette
Musculoskeletal Health and Arthritis: Dr. Jane Aubin
Neurosciences, Mental Health and Addiction: Dr. Anthony Phillips
Nutrition, Metabolism and Diabetes: Dr. Philip M. Sherman
Population and Public Health: Dr. Nancy Edwards
CIHR supports the work of over 13,600 health researchers and trainees
Strategic Outcome(s) and Program Activity Architecture (PAA)
The figure below illustrates CIHR's Program Activity Architecture (PAA) for the 2009-10 fiscal year. It has three Strategic Outcomes divided into nine major Program Activities and 19 Sub-Program Activities.
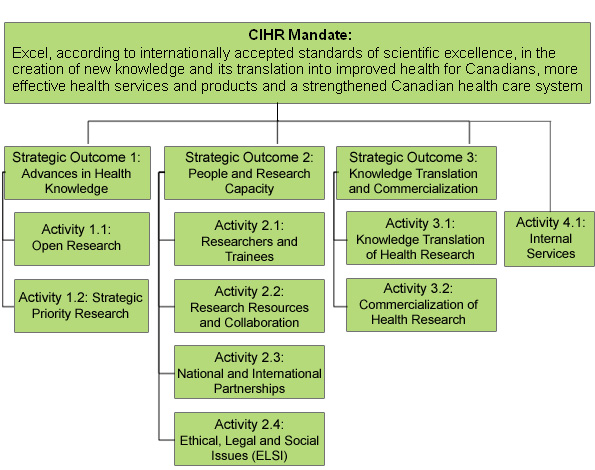
To accomplish its mandate, CIHR provides a range of programs and activities that are designed to support outstanding research, to build health research capacity, and to promote knowledge translation. The following three strategic outcomes and program activities will help position Canada as a world leader in the creation and use of health knowledge for the betterment of Canadians and people across the globe. CIHR's strategic outcomes are as follows:
- Advances in Health Knowledge: Canadian health research advances health knowledge and is responsive to current opportunities and priorities.
- People and Research Capacity: A strong and talented health research community with the capacity to undertake health research.
- Knowledge Translation and Commercialization: Health research is translated and adopted into practice, programs and policies that contribute to more effective health services and products, a strengthened health care system, and the improved health of Canadians.
In 2009-10, CIHR also reported separately on Program Activity 4.1: Internal Services, which include groups of related activities and resources that support the needs of CIHR's programs as well as its other corporate obligations.
Summary of Performance
| Strategic Outcomes | Planned Spending | Total Authorities | Actual Spending |
|---|---|---|---|
| 1.0 Advances in Health Knowledge | $ 591.6 | $ 594.8 | $ 602.2 |
| 2.0 People and ResearchCapacity | $ 291.9 | $ 290.3 | $ 280.7 |
| 3.0 Knowledge Translation and Commercialization | $ 76.1 | $ 76.2 | $ 75.0 |
| 4.1 Internal Services | $ 20.7 | $ 26.4 | $ 25.8 |
| TOTAL | $ 980.3 | $ 987.7 | $ 983.7 |
Total Authorities:
CIHR's total parliamentary authorities increased to $987.7M in 2009-10, an increase of $7.4M compared to its planned spending. This modest increase primarily pertains to transfers received from other federal government departments to strengthen strategic health investments in areas including H1N1 vaccine research, the development of an influenza research network; and, child and
maternal health research.
Actual Spending:
In 2009-10, CIHR's expenditures totaled $983.7M, which was $4.0M less than its total available parliamentary authorities. CIHR lapsed $0.2M of its Grants Vote ($929.3M) during the 2009-10 fiscal year due to diligent resource planning and management. CIHR lapsed $3.8M of its Operating Expenditure Vote ($58.4M); however,
CIHR can carry forward $2.1M of unspent authorities from its Operating Expenditures Vote to the 2010-11 fiscal year.
| Planned | Actual | Difference |
|---|---|---|
| 410 | 396 | 14 |
In 2009-10, the variance in the actual number of FTEs when compared to the number of planned FTEs was mostly attributable to operational slippage including unexpected vacancies, and delays encountered in the hiring process.
Note: CIHR uses a peer review process to identify exemplary projects and individuals that merit funding. In 2009-10, some 2,900 researchers provided their time, without remuneration, and served on peer review panels to review approximately 13,000 applications within a short period of time. Without voluntary support from this community of experts, CIHR would not have the necessary financial and human resources to review and fund the same amount of quality health research.
| Performance Indicators | Targets | 2009-10 Performance |
|---|---|---|
| Canada's rank in the world in health research expenditures. | Maintain or increase international ranking in health research expenditures. |
According to the most recent data from the Organisation for Economic Co-operation and Development (OECD) published in 2009, Canada maintained its position in the top four out of 33 OECD countries in "health-related research and development in government budgets as a percentage of the Gross Domestic Product (GDP)". |
| Changes in health practices, programs or policies informed by CIHR-funded research, improvements in service delivery or health informed by CIHR-funded research. | Anecdotal evidence of changes in health practices, programs, policies, health service delivery, or health due to the work of CIHR funded researchers. |
Reports from the Institutes and other sources show that CIHR-funded research has had a positive impact on health practices, programs, policies and health service delivery. For example:
|
| Research or research agendas informed by CIHR-funded research in Canada and internationally. | Maintain or increase # partnered funding initiatives in Canada and internationally. |
In 2009-10, CIHR actively collaborated with 234 national and international partners to support research on relevant health issues, which provided an additional research contribution of $118M. Compared to 2008-09, CIHR slightly increased its total amount of leveraged funds by partner contributions by 5.9%. Through this collaboration, CIHR is influenced and influences the research agendas of its many partners. |
| Canada's rank in health research publications and patents. | Maintain or increase international ranking in health research publications and patents. | Canada maintained its ranking of 10th in relation to international, medical research publications per billion dollars of Gross Domestic Product (GDP). However, Canada's most recently measured average relative citation (ARC) factor in medical research increased to 1.43 in 2008 from 1.34 in 2007, both of which are well above the global average of 1.0. Although Canada's ARC rating improved from 2007 to 2008, Canada maintains its worldwide ranking of 7th in medical research. |
| Program Activity | 2008-09 Actual Spending |
2009-101 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| 1.1 Open Research | $ 493.9 | $ 449.7 | $ 455.8 | $ 455.6 | $ 473.8 | An Innovative and Knowledge-Based Economy |
|
1.2 Strategic Priority Research |
$ 131.6 | $ 112.0 | $ 135.8 | $ 139.2 | $ 128.4 | |
| Total | $ 625.5 | $ 561.7 | $ 591.6 | $ 594.8 | $ 602.2 | |
1. Commencing in the 2009-10 Estimates cycle, the resources for Program Activity: Internal Service is displayed separately from other program activities; they are no longer distributed among the remaining program activities, as was the case in previous Main Estimates. This has affected the comparability of spending and FTE information by Program Activity between fiscal years. CIHR estimates that $ 16M was spent on Internal Services in 2008-09 for Strategic Outcome #1. This amount is comparable to the amount spent for this Strategic Outcome in 2009-10.
Total Authorities:
Total authorities increased by $33.1M during the year, which was mainly due to a significant portion of the $34M funding increase awarded in the two Program Activities under this Strategic Outcome from Budget 2008 for research that addresses the health priorities of Canadians. The majority of these funds were allocated to key strategic priority research areas including: the next phase of
CIHR's Canadian Longitudinal Study on Aging, the commencement of a unique partnership with the State of California to conduct research into cancer stem cells, safe food and water in northern and aboriginal communities, childhood obesity, and the impact on health of environmental contaminants, all of which support Strategic Priority Research. Additional funding was also
allocated to the Open Research Program Activity to ensure CIHR continues to support Canada's broad base of scientific excellence.
Actual Spending:
Actual spending associated with this strategic outcome was higher than total authorities largely as a result of the re-allocation of funds from Strategic Outcome #2: People and Research Capacity to CIHR's Open Research Program Activity.
| Performance Indicators | Targets | 2009-10 Performance |
|---|---|---|
| Number and types of PhD graduates in Canada by year compared to other countries. | Maintain or increase international ranking. |
According to the most recent data from the Conference Board of Canada, the number of PhD graduates in Canada is increasing slowly, and has increased from 177 per 100,000 population (aged 25-29) to 210 per 100,000 population (aged 25-29) in six years. Despite this increase, Canada’s international ranking in the number of graduated PhD students compared to other OECD countries ranked next to last in 1998, and consistently last from 2005 to 2007. |
| Number of PhD graduates pursuing a postdoctoral fellowship in health research in Canada. | Maintain or increase the number of postdoctoral fellows in health research. |
The number of PhD graduates pursuing a postdoctoral fellowship is an indicator of future health research capacity. In 2007-08, the only year for which CIHR has data, 2,981 PhD graduates pursued postdoctoral fellowships in the medical sciences2. Due to limited resources, CIHR could not collect information on all the parameters listed in the original performance indicator from the 2009-10 Report on Plans and Priorities (RPP): "Percentage of PhD graduates in Canada planning postdoctoral fellowship, research associate-ship or occupation in health/life sciences". However, CIHR is committed to building health research capacity, and increased its number of supported researchers and trainees from 13,021 in 2008-09 to 13,695 in 2009-10. |
| Number and fields of investigators funded. | Maintain number and diversity of investigators funded. |
The number and diversity of investigators funded by CIHR has increased in all research sectors, at all Institutes and for many different types of research. |
| Rating by researchers as to adequacy of resources available for research (infrastructure, resources, hardware, software, people). | 70% or more of researchers rate resources adequate. | Data from the CIHR Open Grants Program evaluation survey completed in 2009 showed that an estimated 91% of CIHR-funded researchers reported they had access to sufficient resources to undertake their research. |
2. Source: The Association of Faculties of Medicine in Canada.
| Program Activity | 2008-09 Actual Spending |
2009-103 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| 2.1 Researchers and Trainees | $ 188.9 | $ 199.7 | $ 214.9 | $ 214.6 | $ 192.0 | An Innovative and Knowledge-Based Economy |
| 2.2 Research Resources and Collaboration | $ 58.9 | $ 48.5 | $ 49.5 | $ 47.9 | $ 60.3 | Healthy Canadians |
| 2.3 National and International Partnerships | $ 23.7 | $ 24.5 | $ 24.7 | $ 24.9 | $ 24.9 | |
| 2.4 Ethical, Legal and Social Issues (ELSI) | $ 2.4 | $ 2.8 | $ 2.8 | $ 2.9 | $ 3.5 | |
| Total | $ 273.9 | $ 275.5 | $ 291.9 | $ 290.3 | $280.7 | |
3. Commencing in the 2009-10 Estimates cycle, the resources for Program Activity: Internal Service is displayed separately from other program activities; they are no longer distributed among the remaining program activities, as was the case in previous Main Estimates. This has affected the comparability of spending and FTE information by Program Activity between fiscal years. CIHR estimates that $ 7.7M was spent on Internal Services in 2008-09 for Strategic Outcome #2. This amount is comparable to the amount spent for this Strategic Outcome in 2009-10.
Total Authorities:
Total authorities increased by $14.8M compared to the 2009-10 Main Estimates. This increase is due to the $14M temporary funding increase announced in Budget 2009 for the CIHR Canada Graduate Scholarships (CGS) Program.
Actual Spending:
Actual spending was less than total authorities due to the in-year re-allocation to the "Advances in Health Knowledge" strategic outcome – more specifically, to the CIHR Open Research Program Activity.
As part of the grants and awards year-end funding strategy, CIHR reviews all programs and initiatives to confirm their forecasted surplus at year-end. In 2009-10, both the Canada Research Chairs Program and the Canada Graduate Scholarships Program were forecasted to have surpluses. These surplus funds were applied to the year-end funding strategy, providing additional funding for new operating grants, as well as additional one-year grants.
| Performance Indicators | Targets | 2009-10 Performance |
|---|---|---|
| Changes in health practice, programs or policies informed by CIHR-funded research, improvements in service delivery or health informed by CIHR-funded research. | Anecdotal evidence of changes in health practices, programs, policies, health service delivery or health due to work of CIHR funded researchers. |
Reports from Institutes and other sources have provided some evidence of the positive impact of CIHR-funded research on health practices, programs, policies and health service delivery. For example:
|
| Commercial activity - products (IP), companies and employment generated as a result of CIHR-funded projects. | Anecdotal evidence of commercial activity due to work of CIHR funded researchers. |
The reports of the Institutes and other sources have provided examples that CIHR-funded research has led to significant commercial activity. For example:
|
| Changes in the health and quality of life of Canadians in areas of CIHR investment. | Maintain or increase international ranking related to quality of life. |
Although it is important to note that health research funded by CIHR could contribute to the improved health of Canadians, we do not attribute the results below to CIHR. Many international studies have shown there are multiple ways to determine Canada's overall health and quality of life status. According to these studies:
|
| Program Activity | 2008-09 Actual Spending |
2009-104 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates |
Planned Spending |
Total Authorities |
Actual Spending |
|||
| 3.1 Knowledge Translation of Health Research | $ 41.5 | $ 40.2 | $ 44.1 | $ 44.0 | $ 45.8 | Healthy Canadians |
| 3.2 Commercialization of Health Research | $ 28.5 | $ 26.1 | $ 32.0 | $ 32.2 | $ 29.2 | An Innovative and Knowledge-Based Economy |
| Total | $ 70.0 | $ 66.3 | $ 76.1 | $ 76.2 | $ 75.0 | |
4. Commencing in the 2009-10 Estimates cycle, the resources for Program Activity: Internal Service is displayed separately from other program activities; they are no longer distributed among the remaining program activities, as was the case in previous Main Estimates. This has affected the comparability of spending and FTE information by Program Activity between fiscal years. CIHR estimates that $ 2M was spent on Internal Services in 2008-09 for Strategic Outcome #3. This amount is comparable to the amount spent for this Strategic Outcome in 2009-10.
Total Authorities:
Total authorities increased by $9.9M compared to the 2009-10 Main Estimates. This increase primarily comes from new funding ($4.4M) approved for the second phase of the Centres of Excellence for Commercialization and Research (CECR) program, and $1.7M of funding for the newly
created Business-Led Centres of Excellence (BL-NCE) program. Both the CECR and the BL-NCE programs, which are reported under the Commercialization of Health Research Program Activity, aim to mobilize
Canada's research talent in the academic, private, public and not-for-profit sectors; and, apply this talent to the task of developing the economy and improving the life of Canadians. These programs are also aligned with the government's science and technology (S&T) strategy: Mobilizing Science and Technology to Canada's Advantage, which provides the framework to guide Canada's S&T policy, and provide Canada an Entrepreneurial Advantage, a Knowledge Advantage and a People Advantage.
The increase to CIHR authorities is also due in part to the $34M base budget increase announced for CIHR as part of Budget 2008. CIHR allocated $3.8M of the $34 base budget increase to various Knowledge Translation and Commercialization activities to facilitate the translation of new knowledge into new products, services or health interventions for the benefit of Canadians.
Actual Spending:
Actual spending associated with this strategic outcome was slightly below planned spending in 2009-10.
Contribution of Priorities to Strategic Outcome(s)
In 2009, CIHR launched its new five-year strategic plan, Health Research Roadmap, which provides a sound foundation and framework for the effective management of key health-related strategic priorities and decisions. Roadmap's strategic directions guide and align efforts in areas of research, knowledge translation and commercialization of health priorities. The operational and management priorities listed in the 2009-10 RPP have been updated in the table below to reflect the wording that was published in the approved Strategic Plan. The status for each priority has also been provided. A three year implementation plan has been developed for the Strategic Plan. It will be published and refreshed annually.
| Operational Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
Strategic Direction #1 |
On-going |
Met All
|
Advances in Health Knowledge And People and Research Capacity |
|
Strategic Direction #2 |
On-going |
Met All
|
All |
|
Strategic Direction #3 |
On-going |
Met All
|
Knowledge Translation and Commercialization |
| Management Priorities | Type | Status | Links to Strategic Outcome(s) |
|---|---|---|---|
|
Strategic Direction #4 |
On-going |
Met All
|
All |
Risk Analysis
CIHR takes a proactive approach to identifying, assessing and managing risks under the broad categories of strategic, operational and corporate risk. In 2009-2010, emphasis was placed on addressing key risks that were identified in its Corporate Risk Profile as well as continuously scanning its environment in order to rapidly identify and mitigate emerging risks.
One of the major risks for CIHR's commitment to improve the health of Canadians through the creation of new knowledge is that health research takes time and often requires sustained, long-term investments to produce its intended results. Meanwhile, CIHR is challenged by the need to provide funding opportunities for new, innovative projects while maintaining previously approved funding for existing projects. To meet this challenge, CIHR engaged in investment modeling to better forecast the future impacts of funding decisions, and to ensure relative stability in the number and proportion of applications funded over time.
Maintaining the appropriate balance between strategic (i.e. targeted) and investigator-initiated (i.e. open) research is also critical to success in health research. Without the appropriate checks and balances in place, there is a risk that CIHR will either miss opportunities to support research addressing emergent or critical health issues; or, miss opportunities to explore new areas of health innovation. Although no single formula exists, CIHR worked to ensure that an appropriate balance was managed through its Governing Council. In 2009-10, Governing Council met numerous times during the year to discuss CIHR's budget, and how to best strategically allocate a portion of available grants to specific programs and priorities. CIHR also engaged a single management committee, chaired by the President of CIHR, to review the results of all grants and awards competitions and to review the proportion of funds allocated to these different competitions to ensure that CIHR's dual objectives of scientific excellence and balance were met.
CIHR supports the creation of new knowledge and its translation into effective health services and products. However, there is a risk that CIHR may not be able to adequately support the synthesis, dissemination, exchange and ethical application of knowledge at the levels required to optimally achieve the knowledge translation component of its mandate. This would result in a lost opportunity to capture the benefits of knowledge translation, which include better health for Canadians, improved health services and products, and economic growth. To meet this challenge, CIHR initiated the development of a knowledge translation strategy in 2009-10, which included objectives, actions and indicators to measure knowledge translation success. The strategy encourages researchers to synthesize and share their results, as well as work directly with other knowledge users to find innovative solutions. Recent changes in the organization have also helped CIHR take on the role of facilitator to promote the synthesis and dissemination of specific research results.
Finally, CIHR must ensure that its operating budget and human resources are allocated optimally to support the achievement of its strategic outcomes. Changes within the organization have helped CIHR take better advantage of its resources and provide the leadership required to successfully implement the strategic directions in the Health Research Road Map. In 2009-10, CIHR developed and launched a new integrated operational planning and budgeting process. This process requires managers to plan activities and identify resource requirements or issues on an annual basis, and reviews progress against these plans on a regular basis.
Expenditure Profile
CIHR Actual Spending Since 2003-04 (in $ millions) 5
5. The expenditure data contained in this chart is based on parliamentary appropriations used. A reconciliation between expenses and parliamentary appropriations used can be found in Note 3 to the CIHR Financial Statements.
CIHR's expenditures increased from $686.2M in 2003-04 to $983.7M in 2009-10, an increase of $297.5M (or 43%) over the past six fiscal years. As illustrated in the table above, however, CIHR expenditures have remained fairly constant since 2007-08. CIHR expects that expenditures for 2010-11 will increase by approximately 2.0%.
Canada's Economic Action Plan (CEAP)
The Government of Canada's 2009 Budget, Canada's Economic Action Plan, provided CIHR with funding to temporarily expand the Canada Graduate Scholarships (CGS) program, which provides financial support to the most outstanding eligible students pursuing Master's or doctoral studies at a Canadian
university. Budget 2009 builds on investments made in previous budgets by providing an additional $14 million for 2009-10. It provided for an additional 200 doctoral scholarships, valued at $35,000 each and an additional 400 master's scholarships valued at $17,500 each.
The CGS program is Sub-Program Activity 2.1.4 under Program Activity 2.1 Researchers and Trainees in CIHR's Program Activity Architecture. More information on the CGS program can be found in Section II.
In 2009-10, Actual Spending exceeded the 2009-10 Main Estimates by $59.4M, due in large part to funding announced for CIHR in the 2008 and 2009 federal budgets which were not included as part of the 2009-10 Main Estimates due to timing issues.
In Budget 2008, the government allocated CIHR a permanent base budget increase of $34M. In Budget 2009, the federal government announced a temporary expansion of the Canada Graduate Scholarships (CGS) program. This expansion of the CGS program enabled CIHR to spend an additional $14M on Canada Graduate Scholarships in 2009-10. CIHR funding approved in Budgets 2008 and 2009 was fully disbursed during the 2009-10 fiscal year.
Several new programs were launched in recent years which further increased CIHR's 2009-10 expenditures. Funding for new programs such as the Drug Safety and Effectiveness Network ($2.1M) and the Business-Led Networks of Centres of Excellence program ($1.7M) were approved as part of the 2009-10 Supplementary Estimates (since they were not included in Main Estimates). Funding for a second round of Centres of Excellence for Commercialization and Research (CECR) grants totalling $4.4M was also approved via the 2009-10 Supplementary Estimates process.
In addition, transfers from other government departments (and other technical adjustments) included in the 2009-10 Supplementary Estimates totalled a net of approximately $3.2M. CIHR often partners with other government departments (e.g. Public Health Agency of Canada, Health Canada) as it recognizes that effective health research needs the collective effort of the many people and organizations committed to making Canadians healthier and to building an effective health care system.