ARCHIVED - Canadian Institutes of Health Research
 This page has been archived.
This page has been archived.
Archived Content
Information identified as archived on the Web is for reference, research or recordkeeping purposes. It has not been altered or updated after the date of archiving. Web pages that are archived on the Web are not subject to the Government of Canada Web Standards. As per the Communications Policy of the Government of Canada, you can request alternate formats on the "Contact Us" page.
2007-08
Departmental Performance Report
Canadian Institutes of Health Research
The original version was signed by
The Honourable Leona Aglukkaq
Minister of Health
Table of Contents
Minister's Message
President's Message
Management Representation Statement
Summary Information
- 1.1 CIHR's Operating Environment
- 1.2 External and Internal Factors Influencing CIHR's Performance in 2007-2008
- 1.3 CIHR's Commitment to Accountability
- 1.4 Alignment to Government of Canada Strategic Outcomes
- 1.5 How CIHR Benefits Canadians
Section II: analysis of program activities by strategic outcome
Strategic Outcome 1.0: Outstanding Research
- Summary of Results
- Program Activity 1.1: Fund Health Research
- Risks and Challenges: Strategic Outcome 1.0
Strategic Outcome 2.0: Outstanding Researchers in Innovative Environments
- Program Activity 2.1: Fund health researchers and trainees
- Program Activity 2.2: Fund research resources, collaboration and other grants to strengthen the health research community
- Program Activity 2.3: Develop and support a strong health research community through national and international alliances and priority setting
- Program Activity 2.4: Inform research, clinical practice and public policy on ethical, legal and social issues (ELSI) related to health and health research
- Risks and Challenges - Strategic Outcome 2.0
Strategic Outcome 3.0: Transforming Health Research into Action
- Program Activity 3.1: Support activities on knowledge translation, exchange, use and strategies to strengthen the health system
- Program Activity 3.2: Support national efforts to capture the economic value for Canada of health research advances made at Canadian institutions
- Risks and Challenges - Strategic Outcome 3.0
Section III: Supplementary Information
Table 5: Departmental Link to Government of Canada Outcome Areas (for DPRs)
Table 6: Comparison of Planned to Actual Spending (including FTEs)
Table 7: Voted and Statutory Items
Table 8: Sources of Respendable and Non-Respendable Revenue
Table 9: Crosswalk - Performance Indicators Used in 2007-2008 RPP vs 2007-2008 DPR
Table 10: Financial Statements
Table 11: Details on Transfer Payment Programs (TPPs)
Table 12: Internal Audits and Evaluations
Section I: Overview
 Minister's Message
Minister's Message
I am very pleased to present the 2007-2008 Departmental Performance Report (DPR) for the Canadian Institutes of Health Research (CIHR).
Last year, the Government of Canada released Mobilizing Science and Technology to Canada's Advantage, a new multi-year strategy designed to build a prosperous economy and promote a better quality of life in Canada through science and technology.
As part of this strategy, we reinforced our commitment to health research. A strong research community not only generates important knowledge, it also leads to improvements in the health of Canadians, strengthens our health-care system, creates new jobs and stimulates economic growth.
CIHR plays a vital role in building and maintaining Canada's thriving health research community. It continues to support world-class Canadian research and has forged strategic partnerships that have maximized the impact of research efforts.
CIHR provides numerous benefits to Canadians. Through its rigorous peer review process, CIHR ensures that the best projects and the brightest researchers are funded. Through its partnerships with industry, CIHR facilitates the acceleration of researchers' findings into commercial applications. Through its innovative knowledge translation programs, CIHR is bringing researchers, clinicians and policy-makers together to translate the results of this research into new health interventions for patients and community health services providers.
The work of Canadian health researchers is already having an impact on the health of people around the globe. Time magazine published its top 10 medical breakthroughs of 2007 and an international research study led by Dr. Stephen Moses, a CIHR-funded researcher, won the coveted first place. Dr. Moses led two clinical trials of male circumcision that proved successful in reducing HIV incidence in young men. CIHR provided over $2.5M in funding to this study.
Canada is just beginning to see the benefits of CIHR's contribution to health research. Its positive impact on the lives of Canadians will be felt for generations to come.
The Honourable Leona Aglukkaq
Minister of Health
Government of Canada
 President's Message
President's Message
This past year, researchers supported by CIHR continued to demonstrate why Canada has a global reputation for scientific excellence. Ensuring research excellence is at the core of CIHR's mandate.
In 2007-2008, CIHR-funded researchers uncovered the genetic roots of autism, creating the possibility of genetic testing to screen for the condition and ensuring early intervention when it is most effective. CIHR-supported researchers developed skin-derived stem cells that have shown great promise for regenerative medicine. CIHR researchers identified risks associated with using antipsychotic medications to treat dementia among the elderly.
This past year, CIHR continued to move ahead with ambitious new programs that address the need for meaningful knowledge translation. One such program is the Partnerships for Health Services Improvement initiative, an exciting new approach that brings researchers and decision-makers together during the research process to improve health systems. Programs such as this will help CIHR provide adaptable health-care solutions that will fit the needs of different jurisdictions across Canada.
Over the past year, CIHR also moved ahead with plans to update Blueprint, CIHR's Strategic Plan. CIHR's Governing Council approved three broad strategies for achieving our mandate: capturing the excellence in the Canadian health research community; addressing research priorities to improve the health of Canadians, support effective health services and products and strengthen our health-care system; and translating knowledge into benefits for health and the economy. Our partners will be critically important in implementing these strategies.
CIHR is at the service of Canada and Canadians. Through the strong and consistent support of the Government of Canada, and its commitment to developing science and technology, CIHR has been able to make significant investments in health research. Collaborations with the private sector, with other federal and provincial funding agencies, with international partners and with health charities have and will continue to intensify the impact of these investments.
CIHR will continue to strive towards building a stronger, more productive health research community in Canada to help improve the health and lives of all Canadians.
Dr. Alain Beaudet, MD, P.h.D.
President, Canadian Institutes of Health Research
Management Representation Statement
I submit for tabling in Parliament, the 2007-2008 Departmental Performance Report for the Canadian Institutes of Health Research.
This document has been prepared based on the reporting principles contained in the Guide for the Preparation of Part III of the 2007-2008 Estimates: Reports on Plans and Priorities and Departmental Performance Reports:
- It adheres to the specific reporting requirements outlined in the Treasury Board Secretariat guidance;
- It is based on the department's approved Strategic Outcome(s) and Program Activity Architecture that were approved by the Treasury Board;
- It presents consistent, comprehensive, balanced and reliable information;
- It provides a basis of accountability for the results achieved with the resources and authorities entrusted to it; and
- It reports finances based on approved numbers from the Estimates and the Public Accounts of Canada.
Name: Dr. Alain Beaudet, MD, P.h.D.
Title: President, Canadian Institutes of Health Research
Summary Information
CIHR's Mandate
The mandate of CIHR is to excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health- care system (Bill C-13, April 13, 2000).
To accomplish its mandate, CIHR provides a range of programs and activities that are designed to support outstanding research, both investigator-driven and strategic or targeted, to build health research capacity and to promote knowledge translation. CIHR funds nearly 12,000 health researchers and trainees in universities, teaching hospitals and other health organizations and research centres across the country who conduct research in the following areas: biomedical; clinical; health systems and services; and the health of populations, societal and cultural dimensions of health and environmental influences on health. It funds health research that meets the highest international standards of excellence and ethics. Together, these activities will position Canada as a world leader in the creation and use of health knowledge for the betterment of Canadians and people across the globe.
Financial Resources ($M)
| 2007-2008 | ||
|---|---|---|
|
Planned Spending $869.5 |
Total Authorities $993.7 |
Actual Spending $974.1 |
Human Resources
| 2007-2008 | ||
|---|---|---|
|
Planned 406 |
Actual 361 |
Difference 45 |
CIHR's Program Activity Architecture (PAA)
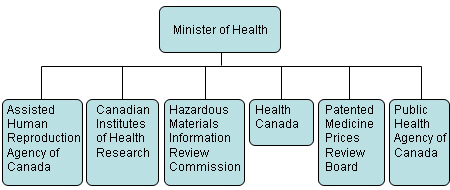
CIHR's Departmental Report Program Activity Architecture (PAA) as approved by Treasury Board is shown in Figure 1 below. The PAA consists of three Strategic
Outcomes and the key program activities that support CIHR's Strategic Outcomes. The performance information presented in Section II is organized according to this PAA
structure. Please note that CIHR's PAA was revised in 2007-2008 according to TBS guidelines in order to better reflect how CIHR
funds research to meet its mandate. As these changes took effect on April 1, 2008 they are not reflected in this document.
Figure 1: CIHR's Program Activity Architecture (PAA)

Summary of CIHR's Performance for 2007-2008
In its 2007-2008 Report on Plans and Priorities (RPP), CIHR committed to the priorities and related investments described in the tables below. These tables provide a summary of how CIHR performed relative to expected results and priorities. Finally, they provide a comparison of planned and actual spending in each Strategic Outcome. It should be noted that the linkages between health research inputs, outputs and impacts are difficult to trace when knowledge develops incrementally over an extended period of time and through multiple channels. Attribution of credit for research impacts can also be complex, as impacts often result from a number of research projects carried out or funded either collaboratively or independently in the same and/or different countries. As such, this report provides only limited performance information relating to the outcomes and impacts of CIHR funded research. CIHR is committed to measuring and reporting on the outcomes of its funded activities. For example, in 2007-2008 CIHR began the development of a Research Reporting System to systematically collect information on the results and impacts of funded research.
As outlined in Tables 1 & 2 and described in more detail in Section II of this report, CIHR has made significant progress in the priority areas and has successfully met the expected results and planned spending for all but one of its program activities. This performance status was primarily determined based on an assessment of planned and actual spending levels, activities, and outputs rather than an in depth assessment of efficiency and effectiveness.
Efficiency is measured at the organizational rather than the program activity level as most programs share common business processes and systems. CIHR considers itself efficient as its administrative costs have been consistently below its target of 6% of its annual budget (4.8% in 2007-2008) and so well below the norms in the federal government. This achievement is a reflection of CIHR's extensive use of automation to electronically collect and process applications and the more than 2,000 researchers who contribute, on average, three weeks of their time each year without remuneration to serve on more than 130 peer review committees.
CIHR assesses the effectiveness of its programs largely through evaluation. Over the past eight years it has conducted some 21 evaluations and collaborated on an additional six Tri-agency evaluations. In addition, as required by its legislation, CIHR underwent in 2006 a comprehensive assessment by an international review panel composed of 27 eminent scientists and other professionals led by Dr. John Bell, the Regius Professor of Medicine at Oxford University. For the most part, these studies have concluded that the programs are contributing as expected to program objectives and have recommended a variety of program adjustments to improve performance. The International Review Panel, for example, concluded that, "The accomplishments of the CIHR to date are many and virtually every aspect of the mandates has been significantly developed…Many of [its] activities provide novel and potentially very interesting and productive approaches towards making health research both more effective and more relevant…It is likely that this model will provide important new research outputs relevant to human health". While we acknowledge that we do not have evaluation results to support an in-depth assessment of all of our programs, CIHR recently finalized its five year evaluation plan which will ensure that all of its programs will be evaluated by 2012-2013. Evaluation findings will be presented in future reports.
In one case CIHR has not met expected results. This is for Program Activity 2.4 'Inform research, clinical practice and public policy on ethical legal and social issues related to health and health research'. For this program activity actual spending was significantly less than planned. This was a reflection of the lack of capacity for ethics research in Canada. While programming in this area has over time helped to build this capability, the community of interested and capable researchers remains too small to fully utilize the available funding. Note that the underutilized funds were transferred during the year to other priority areas.
In one case CIHR has exceeded expected results. This is for Program Activity 3.2 'Support national efforts to capture the economic value for Canada of health research advances made at Canadian institutions'. For this program activity the actual spending, activity and outputs were significantly higher than planned. Budget 2007 announced $163M of funding for the new Centres for Excellence for Commercialization and Research (CECR) program. This innovative program invests in the establishment of research and commercialization centres capable of achieving global leadership in Canada. Funding was allocated to the three granting councils based on the results of the inaugural competition with the result that CIHR received $73.5M of additional funding in the period.
Table 1: Departmental Priorities
Name |
Type |
Performance Status |
|---|---|---|
|
Strategic Priority No. 1: |
Ongoing |
Successfully met* |
|
Strategic Priority No. 2: |
Ongoing |
Successfully met* |
|
Strategic Priority No. 3: |
Ongoing |
Successfully met* |
*As these are ongoing priorities, "successfully met" is intended to indicate that significant progress has been made in the priority areas. This assessment is based on the best available evidence that expected results for 2007-2008 are being achieved in the majority of the program activities that contribute to the priority area. The performance status for each of the program activities is outlined in Table 2.
Table 2: Program Activities by Strategic Outcome
| Program Activity | Expected Results | Performance Status | 2007-2008 | Contributes to the following priority | |
|
Planned Spending ($M) |
Actual Spending ($M) |
||||
| Strategic Outcome 1.0: Outstanding Research - Best health research supported to create health knowledge responding to opportunities and priorities | |||||
| 1.1. Fund health research | Effective and efficient funding programs that enable ethical health research, responding to opportunities and priorities | Successfully met | $493.5M | $539.5M |
Strategic Priority No. 1 |
| Strategic Outcome 2.0: Outstanding Researchers in Innovative Environments - Strong health research community able to undertake outstanding research | |||||
| 2.1. Fund health researchers and trainees | Effective and efficient funding programs that ensure a supply of highly qualified health researchers and trainees are available to conduct outstanding research. | Successfully met | $203.6M | $202.3M |
Strategic Priority No. 2 |
| 2.2. Fund research resources, collaboration and other grants to strengthen the health research community | Effective and efficient partnerships and funding programs that lead to a dynamic research environment and enable outstanding research. | Successfully met | $70.0M | $68.0M |
Strategic Priority No. 2 |
| 2.3. Develop and support a strong health research community through national and international alliances and priority setting | National and international health research agendas are formulated and implemented. | Successfully met | $28.1M | $24.0M |
Strategic Priority No. 2 |
| 2.4. Inform research, clinical practice and public policy on ethical, legal and social issues (ELSI) related to health and health research | Uptake and application of ethics knowledge as an integral part of decision-making in health practice, research and policy. | Not met | $6.3M | $2.2M |
Strategic Priority No. 2 |
| Strategic Outcome 3.0: Transforming Health Research into Action - Health research adopted into practice, programs and policies for a productive health system; and stimulation of economic development through discovery and innovation | |||||
| 3.1. Support activities on knowledge translation, exchange, use and strategies to strengthen the health system | Effective dissemination, exchange, synthesis and application of research results take place to create new knowledge, strengthen Canadian capacity and networks, and together with our partners, enable effective research and knowledge translation of health research. | Successfully met | $40.7M | $39.8M |
Strategic Priority No. 3 |
| 3.2. Support national efforts to capture the economic value for Canada of health research advances made at Canadian institutions | Mobilizing research to improve health services, products, a strengthened healthcare system and the economy. | Exceeded expectations | $27.3M | $98.3M |
Strategic Priority No. 3 |
1.1 CIHR's Operating Environment
Approach to Health Research
CIHR's vision is to position Canada as a world leader in the creation and use of new knowledge through health research that benefits the health of Canadians and the global community.
CIHR's 13 Institutes
CIHR is made up of 13 Institutes, each of which addresses a health research theme that is of importance to Canadians and helps set health research priorities for CIHR. As enshrined in its legislation in 2000, these are virtual and temporary institutes, attached to a university or teaching hospital, rather than a permanent brick and mortar office. This organizational structure is unique in the world and provides the Institutes with the flexibility needed to be responsive and effective and facilitates a direct connection to the research community.
Each of CIHR's 13 Institutes is headed by a Scientific Director who is a recognized expert in his or her field and within the research community. Each Institute receives guidance from its Institute Advisory Board made up of health stakeholders, including other research funders, researchers and research users and representatives of the private and non-profit sectors.
CIHR uses a problem-based, multidisciplinary and collaborative approach to health research. Through its Institutes, CIHR is creating new opportunities for Canadian health researchers to produce results that matter to Canadians and the rest of the world.
|
CIHR Institutes Aboriginal Peoples' Health (IAPH) |
A Key Role in the Health Portfolio
The Health Portfolio is the focal point for the Government of Canada's health-related activity. It is comprised of six entities with distinct but complementary mandates, including CIHR.
As Canada's health research funding agency, CIHR makes an essential contribution to the Minister of Health's overall responsibilities by funding the research and knowledge translation
needed to inform the evolution of Canadian health policy and regulation. This is achieved through an extensive and growing set of linkages with branches throughout Health Canada and the Public Health
Agency of Canada, which provide Portfolio decision-makers with access to high quality and timely health research knowledge.
The Health Portfolio consists of approximately 11,700 employees and an annual budget of over $4.5B.
Federal Funding Agency Collaboration
CIHR works closely with other federal funding agencies - the Natural Sciences and Engineering Research Council (NSERC), the Social Sciences and Humanities Research Council (SSHRC) and the Canada Foundation for Innovation (CFI) to create
inter-agency mechanisms that foster a more comprehensive approach to the overall management of research support. Specific inter-agency initiatives are also underway to support the implementation of the
Federal Science and Technology Strategy. The agencies have established senior-level mechanisms for ongoing planning and exchange, the harmonization of policies and practices, and the collaborative delivery
of programs. A detailed inter-agency report and action plan was presented to the Ministers of Health and Industry in January 2008.
CIHR's Core Business
CIHR activities include the funding, coordination and promotion of health research through open competitions, strategic initiatives, and knowledge translation. CIHR
funds two kinds of research: open and strategic (also known as targeted). In open research, scientists are left to choose what they propose to research, as they are in the best position to know what lines
of discovery are most likely to yield advances. Open research is the foundation for scientific advancement because it lets the best new ideas come to the forefront.
In strategic research, CIHR selects areas of priority in response to the concerns of citizens, experts, governments and other stakeholders, and calls upon the research community to propose projects in those areas. CIHR also uses strategic research when it wishes to improve the strength of the research community in an area where expertise is lacking; for example, in the case of emerging new technologies, or to seize an opportunity to position Canada for world leadership.
In order to deliver on CIHR's mandate it is evident that the health research enterprise in Canada must be strong. Canada needs a continuing supply of highly qualified personnel to carry out research in Canada's universities, hospitals and other research institutions. CIHR has training and salary programs to support the development of the very best researchers during the different stages of their careers.
Knowledge Translation
A key part of CIHR's mandate, knowledge translation (KT) is a dynamic and iterative process that includes synthesis, dissemination,
exchange and ethically sound application of knowledge to improve the health of Canadians, provide more effective health services and products and strengthen the health care system. This is accomplished
through the funding of knowledge translation research and activities; facilitation and management of partnerships that can accelerate knowledge translation; and the development of measurement, analysis
and evaluation policies, frameworks and tools to assess the outcomes and impacts of CIHR-funded research.
Commercialization
Commercialization is an integral part of CIHR's KT mandate. To help achieve this mandate, CIHR has developed programs designed to facilitate the
movement of health research discoveries from the academic setting to the marketplace.
CIHR's Partnerships - Leveraging our Impact
In addition to funding research, developing scientists and enabling the use of research results, CIHR creates synergies in health research by bringing people and institutions together
into networks and collaborative efforts so they can be more effective than on their own.
CIHR also collaborates with others to increase the impact of its activities. Partners provide access to different audiences, thereby ensuring more opportunities to communicate the benefits of research to Canadians. CIHR works jointly with hundreds of organizations, including the Bill and Melinda Gates Foundation and both large and small voluntary health organizations, such as the Heart and Stroke Foundation of Canada and private sector organizations including pharmaceutical manufacturers.
In the eight years that CIHR has been in existence, it has established more than 830 partnership agreements with over 400 organizations. Over this same period, these partnerships have leveraged more than $716.2M in additional funding for CIHR-led health research projects1. But partners' contributions are not measured solely in financial terms. They play a key role in helping to set research priorities and in developing programs and initiatives that help meet those priorities.
- Partner contributions are likely understated as the figures do not include "in-kind" partner contributions and some partner funds that are not administered by CIHR.
International Collaborations2
Since its inception in 2000, CIHR has developed strong collaborative relations with sister organizations in various countries in Africa,
Asia-Pacific, Europe and the Americas. To date, CIHR has established over 150 partnerships and joint collaborations, each bringing together teams of leading Canadian and international
researchers to work on health research issues of mutual importance and benefit. Through its Grants and Awards programs, CIHR has funded over 2,300 research projects with international
linkages, all aimed at tackling health issues of critical importance to Canada and the world at large.
World Class Research Through CIHR's Peer Review Process
CIHR's peer review system ensures that CIHR's funding process is fair and open, that taxpayers' money is spent wisely, and that the best and brightest researchers
are funded. Applications for support from CIHR undergo a rigorous peer review process by committees of experts in their field. These experts examine proposals with respect to their
significance in advancing knowledge and promoting the health of Canadians. In 2007-2008 there were nearly 130 CIHR peer review committees. The peer review process involved over 2,000
expert reviewers each year from Canada and abroad who volunteered an average of 15 days of their time per year.
2. International linkages include any funded grants where at least one of the research team members declared that they belong to a primary institution and/or research institution of the project which is outside Canada and includes any awards held by awardees whose primary institution and/or research institution of the project was declared as being outside Canada. It also includes all funded grants/awards on a predefined list of international initiatives.
1.2 External and Internal Factors Influencing CIHR's Performance in 2007-2008
Several external and internal factors influenced CIHR's overall performance in 2007-2008 such as:
1. S&T Strategy 'Mobilizing Science and Technology to Canada's Advantage'
In May 2007, the Government's Science and Technology Strategy "Mobilizing Science and Technology to Canada's Advantage" was released, seeking to ensure that public policy and expenditures
are strategic, efficient and accountable, deliver results, and make a difference in the lives of Canadians. The Tri-agencies - CIHR, the Social Science and Humanities Research Council
(SSHRC) and the Natural Sciences and Engineering Research Council (NSERC) - in conjunction with the Canada Foundation for Innovation (CFI)
have worked together over the past year to respond to the policy objectives of the S&T Strategy. The Tri-agencies focused on two priorities in 2007-2008:
a) Rapid and effective design and delivery of programs that reflect the S&T Strategy objectives. For example, the Tri-agencies collaborated to create a new Private Sector Advisory Board and launch the new Centres of Excellence for Research and Commercialization (CECR) program in June 2007 with the first competition completed by February 2008.
b) The creation of inter-agency mechanisms that foster a more comprehensive approach to the overall management of research support. The Tri-agencies and CFI completed a baseline analysis of the evolution of federal investments to university-based research and initiated consultations with external stakeholders on this topic.
CIHR contributes directly to each of the three advantages of the strategy as follows:
Knowledge Advantage
CIHR is investing in health research in areas of Canadian strength and is building multidisciplinary research teams to tackle complex health problems. Together, CIHR
and NSERC have doubled investments in their joint program 'Collaborative Health Research Projects' (CHRP) which aims to bring researchers in the fields of natural sciences and engineering together with the health sciences for greater health and
economic benefits.
Entrepreneurial Advantage
CIHR is increasing its emphasis on the translation of new knowledge into practical applications and concrete benefits for Canadians through its knowledge translation and commercialization
programs. In September 2007, CIHR launched its new Policy on Access to Research Outputs. The policy which took effect January 1, 2008 encourages CIHR-funded
researchers to ensure that their original research articles are freely available online within six months of publication.
People Advantage
CIHR's training, scholarship and Research Chairs programs contribute to attracting and retaining the highly skilled people that Canada needs to thrive in the global economy.
CIHR's Canada-China Norman Bethune Health Research Scholarships will bring Chinese scholars to study at the PhD level in Canadian institutions.
2. Recommendations from CIHR's 5 Year Review
In June 2006, the International Review Panel (IRP) responsible for CIHR's first 5 year performance review delivered its final
report which applauded CIHR's accomplishments to date and identified key areas for improvement. Many of these improvements were made in 2007-2008. CIHR will continue
to address the remaining ones in 2008-2009 and beyond as part of its second strategic planning and priority-setting exercise, known as Blueprint II.
3. Renewal of CIHR's Strategic Plan: Blueprint II
In January 2004, CIHR launched its first four-year strategic plan: Investing in Canada's Future: CIHR's Blueprint for Health Research and Innovation. In
2007-2008 CIHR began the process of renewing and revising its strategic plan to create Blueprint II which will build on lessons learned from CIHR's first
7 years and the recommendations provided by the IRP. The direction for Blueprint II is set by CIHR's Governing Council, which will approve the overall plan
and monitor alignment of CIHR activities and progress. In developing the plan, CIHR will harmonize its strategic directions and research and knowledge translation
priorities with overall Government policy, such as government health priorities, the S&T Strategy and the Speech from the Throne. The strategic planning process will include national consultations with
CIHR's partners and health research stakeholders. A five year investment strategy will be developed to support its implementation.
4. Change in Leadership
After seven years as CIHR's inaugural President, Dr. Alan Bernstein stepped down in November 2007. Dr. Bernstein's exceptional leadership to CIHR and the health research
community during his tenure strongly influenced CIHR's success to date. Dr. Pierre Chartrand, the Vice-President of CIHR's Research Portfolio, was appointed as Acting
President of CIHR while the search for a new president was conducted. In March 2008, Dr. Alain Beaudet, a Montreal physician, neuroscience researcher and President and Chief Executive
Officer of the Fonds de la recherche en sant� du Qu�bec (FRSQ) since 2004, was named as CIHR's new President effective
July 1, 2008.
5. CIHR's Key Risks
Since its inception, CIHR has experienced significant growth. Sustained government investment in health research over the past decade has enabled Canada to capitalize on advances in
biology and medicine, has supported important Canadian health discoveries in recent years and secured Canada's place on the global stage. As CIHR strives towards fully meeting its mandate,
it has been evolving from a granting council to a mature health research and knowledge translation organization. This has occurred with the guidance of the results of the International Review Panel Report.
There are a number of risks associated with this transformation. These risks need to be mitigated so that CIHR can be successful and effective and can ensure that it is able to demonstrate
the impact of investments in health research.
In this section the more significant strategic risks for CIHR have been highlighted. Where possible the impact and likelihood of the risks as well as mitigation strategies that have been put into place are described. A number of more specific, operational risks that affect CIHR's programming are also described and linked to CIHR's strategic outcomes in other sections of the document.
Risk # 1: Optimal allocation of research funds: There is a risk that CIHR funds are not optimally allocated to support the achievement of its strategic outcomes.
Impact: This could result in eligible research opportunities that are well aligned to government priorities going unfunded, large strategic initiatives being underfunded and thus not having a significant impact, and could affect the long-term sustainability of the health research capacity in Canada.
Mitigation: A number of advisory and governing committees have been put in place to ensure the optimal allocation of research funding. For example, the CIHR Research and Knowledge Translation Committee (RKTC) which includes the President, the Scientific Directors and a number of other key executives is responsible, as delegated by Governing Council, for all research-related decision-making including funding decisions . This is supported by a Strategic Investment Proposal process which requires that all new investment proposals demonstrate alignment, impact and sustainability.
Risk # 2: Effectiveness of CIHR programming: There is a risk that CIHR programs are not designed to effectively develop and translate health research knowledge and to increase health research capacity in Canada.
Impact: Health research is the source of new knowledge about human health including how to maintain optimal health; how to prevent, diagnose, and treat disease; and how to manage the health care system. Ineffective programming could limit the development of new knowledge and advances in health research and limit the ability to attract, develop and sustain a strong research community. This would ultimately affect CIHR's ability to improve the health of Canadians, introduce more effective health services and products and strengthen the Canadian health care system.
Mitigation: To mitigate this risk, CIHR has significantly increased its evaluation capacity and developed a long term evaluation plan so that all CIHR programming is evaluated at least once in a five year period. CIHR is also in the process of developing a program design control framework that will ensure that best practices, lessons learned and evaluation results are considered in the design of new programs.
Risk # 3: Sustainability of the funding model for operations: There is a risk that CIHR's current funding model for operations limits the organization's ability to continue to increase its internal capability, enhance its processes and systems and strengthen internal controls to improve effectiveness, respond to central agency requirements and increase its overall accountability and transparency.
Impact: This could result in: an inability to attract and retain resources with the right level of skills and experience; poor financial controls; and an inability to develop the processes, information and tools to support effective management and decision making.
Mitigation: To mitigate this risk CIHR has implemented an integrated operational planning process which requires managers to plan activities and identify resource requirements or issues on an annual basis and a process to review progress against these plans on a quarterly basis. CIHR is also in the process of developing a five year operational "roadmap" which will provide a vision for the on-going evolution of CIHR's operations together with an assessment of the funds required to support operations in the future and funding strategies to realize the vision.
1.3 CIHR's Commitment to Accountability
The following includes some of the activities undertaken by CIHR in 2007-2008 which demonstrates its commitment to being accountable to Canadians and to ensure that its programs and investments have the maximum positive impact possible on Canadian society and on research internationally.
Measuring and Reporting on the Impacts of Research
Measuring and reporting on performance is critical both in terms of meeting CIHR's commitment to be accountable to Canadians and to ensure that our programs and investments have the
maximum possible positive impact in Canada and internationally. CIHR understands the importance of measuring performance at multiple levels - organizational performance, program performance
and the performance and results of the health research itself. However, measuring the impacts of health research investments is a challenge; countries around the world are grappling with this issue.
CIHR has created, published and presented, both nationally and internationally, a framework for assessing the impact of the research it funds and is working with other granting councils on a shared framework for reporting on impact. CIHR's framework outlines five categories of research impact (Advancing Knowledge, Building Capacity, Informing Decision-Making, Health Impacts and Economic Impacts). CIHR will be better able to report more comprehensively on two of the categories of the more short-term impacts such as advancing knowledge and creating research capacity with the advent of CIHR's new research reporting system to be launched in 2009. As well, several special studies are underway to capture and report on longer term categories of impact; namely: the use of health research to inform decisions, as well as health and economic impacts.
Strengthened Evaluation and Analysis Capacity
CIHR has invested significantly in strengthening its evaluation and analysis capacity, including analytical expertise on measuring the impacts of health research. As well, in 2007-2008
CIHR's Evaluation group worked towards developing a 5-year Evaluation Plan as a key step towards fulfilling Treasury Board's requirements for corporate evaluation under the proposed
new Federal Evaluation Policy. In developing this 5-year plan, CIHR is being proactive in preparing to meet the accountability and reporting requirements of the Federal Government once
the new Evaluation Policy is approved in the fall of 2008.
Research Reporting System
In 2007-2008 CIHR began the development of a Research Reporting System (RRS) to address the need for improved performance reporting.
The RRS will facilitate the systematic collection, synthesis and reporting of health research results and their impacts. It will provide data that is critical to CIHR
for performance monitoring, analysis and evaluation. In 2008-2009 CIHR will begin to implement its End-of-Grant Reporting policy which will require that researchers document the outputs
and impacts of their research.
Policy on Access to Research Outputs
In September 2007, CIHR unveiled its new policy 'Access to Research Outputs'. Under this Policy, which will apply to all CIHR grants awarded after January 1, 2008,
grant recipients must make every effort to ensure that their peer-reviewed research articles are freely available as soon as possible after publication. Open access enables authors to reach a much broader
audience, which has the potential to increase the impact of their research. From a knowledge translation perspective, this policy will support CIHR's strategic priority to expedite
awareness of and facilitate the use of research findings by policy makers, health-care administrators, clinicians, and the public, by greatly increasing ease of access to research. This policy builds
on other important initiatives to promote the openness and transparency of CIHR-funded research such as the registration of clinical and randomized controlled trials.
Community Reviewers Program
CIHR is committed to enhancing public engagement in health research in Canada. One of the mechanisms to accomplish this goal is through inviting Community Reviewers to sit on
CIHR's peer review panels. These reviewers are members of the public who are not currently involved in academia or research, but who have a demonstrated interest in health and science.
This program provides a mechanism for public accountability, increases transparency of CIHR's peer review process, and communicates the merits of investment in health research to the
public and stakeholders. With support from key stakeholders including the Chairs of CIHR's peer review panels, the number of community reviewers increased from 7 in 2006-2007 to 15
in 2007-2008. These community reviewers participated in 20 peer review meetings within the Open Operating Grants Program and reviewed more than 600 lay abstracts.
1.4 Alignment to Government of Canada Strategic Outcomes
Health research is directly linked to the Government of Canada's commitments to improving the health of Canadians and building an innovative and knowledge-based economy. The following table illustrates how CIHR's Strategic Outcomes and key program activities align to and support the Government of Canada Strategic Outcomes:
Table 3: Alignment to Government of Canada Strategic Outcomes
| CIHR Strategic Outcome | CIHR Program Activity | Alignment to Government of Canada Strategic Outcomes | Explanation of Alignment |
|---|---|---|---|
| 1. Outstanding Research | 1.1 Fund health research | Economic: An innovative and knowledge-based economy | Through investments in both innovative research, as well as career and salary support for top Canadian researchers, CIHR is building a 21st Century research plan that will help realize Canada's knowledge advantage. |
| 2. Outstanding Researchers in Innovative Environments | 2.1 Fund health researchers and trainees | Economic: An innovative and knowledge-based economy | CIHR is an integral partner in implementing the People Advantage in the Government's S&T Strategy and recognizes that talented, skilled, creative people are the most critical element of a successful national economy. |
| 2.2 Fund research resources, collaboration and other grants to strengthen the health research community | Social: Healthy Canadians with access to quality health care | CIHR is mandated to excel in the creation of new knowledge and its translation into benefits for Canadians; this is accomplished in part through nurturing partnerships with the business, academic, and public sectors. | |
| 2.3 Develop and support a strong health research community through national and international alliances and priority setting | Social: Healthy Canadians with access to quality health care | CIHR's 13 Institutes are bringing together research funders, researchers and knowledge users (including policy-makers and practitioners) to set strategic priorities for research, reflecting Government science priorities to improve the health of Canadians and our health care system. | |
| 2.4 Inform research, clinical practice and public policy on ethical, social and legal issues (ELSI) related to health and health research | Social: Healthy Canadians with access to quality health care | CIHR is nurturing a research environment that is founded on world-class excellence across the full spectrum of health research - from basic science to health services and policy. | |
| 3. Transforming Health Research into Action | 3.1 Support activities on knowledge translation, exchange, use and strategies to strengthen the health system | Social: Healthy Canadians with access to quality health care | CIHR is emphasizing knowledge translation to advance the use of research to support health and strengthen Canada's health- care system, thereby reflecting the S&T Strategy's principle to apply the benefits of research to all Canadians. |
| 3.2 Support national efforts to capture the economic value for Canada of health research advances made at Canadian institutions | Economic: An innovative and knowledge-based economy | Implementation of commercialization activities will ensure that CIHR's work is aligned with Canada's Entrepreneurial Advantage, which encourages the translation of research into practical applications that will improve health, the health care system and strengthen the economy. |
1.5 How CIHR Benefits Canadians
Canadians understand that health research has provided the remarkable advances in health sciences that have taken place in the last few decades. Health research supported by the former Medical Research Council (MRC) and then by CIHR has yielded many health benefits for Canadians such as improved diagnostic methods, drugs, treatment methods, surgical techniques and an improved health care system. CIHR's activities are directly relevant to the needs of Canadians, which include:
- The need to reduce the effects of disease and illness which can include reduced life expectancy, lower quality of life and lost productivity. Research finds treatments to mitigate these impacts.
- The need to respond quickly and effectively to health crises such as outbreaks of infectious diseases. Researchers can be rapidly mobilized to address these, as seen during the SARS crisis.
- The need to improve the cost-effectiveness of our health system. Research can help identify innovative and cost-effective ways of providing health services.
- The requirement of government for evidence to guide its policy and regulatory decisions. For example, research can provide the evidence required to establish wait time targets or whether a particular drug is unsafe or ineffective.
- The need to carry out research in an ethical way, particularly when it involves human subjects - for example, CIHR has developed a first set of ethical guidelines for federally-funded research in Canada involving Aboriginal people.
- The need for leadership on complex challenges such as the growing burden of obesity and mental health in the workplace. CIHR has launched a number of major initiatives to address them, in collaboration with the public, voluntary and private sectors, both domestically and internationally.
Section II: Analysis Of Program Activities By Strategic Outcome
Note on Information Sources
The information presented in this Departmental Performance Report is drawn from a variety of sources. CIHR's Electronic Information System (EIS) provides data on the number and value of project awards under the various funding programs.
A second source is the results of a survey of funded and non-funded researchers conducted for CIHR by EKOS Research Associates in February and March 2005. Both surveys involved structured telephone interviews. A total of 1,676 interviews were completed with respondents coming from a broad range of disciplines and located across the country. This survey provides valuable information on the perspectives of researchers; a key stakeholder group, towards CIHR's many activities. Further information on this survey can be found at http://www.cihr-irsc.gc.ca/e/31683.html.
A third source is the results of program evaluation studies conducted on CIHR's Institutes and programs. More information, including methodology and detailed results for these evaluations, can be found at http://www.cihr-irsc.gc.ca/e/31683.html.
A fourth source is the International Review Panel Report, published in June 2006. The report can be found at: http://www.cihr-irsc.gc.ca/e/documents/irp_2000-2005_e.pdf.
Organization of Performance and Results Information
The following sections are organized by each of CIHR's three Strategic Outcomes. First, an overview of the Strategic Outcome and its indicators is presented, along with some macro-level performance data. Then, each Program Activity under the Strategic Outcome is presented with an assessment its performance based on a comparison of planned and actual spending, activities, and outputs. Finally, each Strategic Outcome section concludes with a summary of relevant risks and challenges.
CIHR continues to make modifications to the set of performance indicators used to monitor its various program activities and sub-activities. In some cases the indicators used differ from those identified in the 2007-2008 RPP due to the availability of performance data or concerns that the data was not reliable. However, the indicators used in this report are consistent with those used in the DPR for 2006-2007. A crosswalk table comparing these indicators to the indicators used in the 2007-2008 RPP is provided under Section III: Supplementary Information.
As outlined in Section 1.3, CIHR is committed to measuring and reporting on performance and work is underway to improve both the indicators and the data available to report against the strategic outcomes and program activities in the PAA.
Strategic Outcome 1.0: Outstanding Research
CIHR's Strategic Outcome 1.0 ensures that:
World-class health research, responding to research opportunities (investigator-framed) and priorities (institute-framed) is funded to create health knowledge.
Enabling the conduct of outstanding research is the largest part of CIHR's core business. Throughout 2007-2008, CIHR continued to ensure that the best health research across all disciplines was supported in order to create health knowledge responding to opportunities and federal government priorities.
Summary of Results
Three measurement indicators are used to monitor CIHR's performance against this strategic outcome:
- Canadian ranking in health research expenditures compared to international levels;
- Number of publications resulting from CIHR-supported research and their impact; and
- Rating the quality of results of CIHR-funded research.
One of the key enabling inputs for health research is the amount available for investment. CIHR therefore monitors international trends regarding the level of investment in research in general and health research in particular. The number of publications resulting from CIHR-funded research is also an indicator of the overall productivity of Canadian researchers. Finally, rating the quality of results of CIHR-funded research is an indicator of the quality of the outputs of investment in research. It is important to note that CIHR is not the only organization that contributes to the achievement of this strategic outcome. Support for health researchers is also provided through other Canadian provincial and federal granting agencies for example: FRSQ, SSHRC and NSERC. Therefore, CIHR does not claim direct attribution for the results.
1. Canadian ranking in health research expenditures compared to international levels
The Canadian government is the second-largest funder of general research and development (R&D) in Canada, behind the business sector. Since the end of the 1990s, federal expenditures have increased steadily, mostly through the funding of the higher-education system and via the federal granting Tri-Agencies (CIHR, SSHRC and NSERC) as well as the National Research Council, the Department of National Defence, the Canada Foundation for Innovation (CFI) and Genome Canada, etc. However, total government funding for R&D in Canada still trails the United States and other Organizations for Economic Co-operation and Development (OECD) countries.3 OECD data indicate that Canada currently ranks 12th out of 30 countries in terms of the share of Gross Domestic Product (GDP) invested in overall R&D.4 Federal Government investment in Health-related R&D (as a % of GDP) between 2000 and 2006 continues to rank Canada in the top five OECD countries (Figure 2).
3. "Science and technology Policy Documents", Science and Technology Data - 2004 available at http://strategis.ic.gc.ca/epic/site/rti-rti.nsf/en/te04319e.html
4. See OECD, Main Science and Technology Indicators, 2006 http://www.oecd.org/dataoecd/49/45/24236156.pdf.
Figure 2: Health-related R&D in government budget as a percentage of GDP, 2006
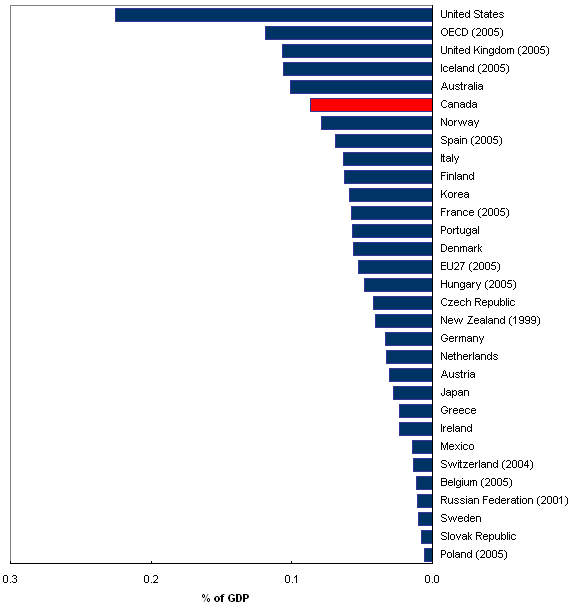
Source: OECD, R&D database, May 2007
2. Number of publications resulting from CIHR-supported research and their impact
Publications are a key output measure of the productivity of researchers and a primary method by which the outcomes of research are translated into results for Canadians. There are two key factors: the overall number of publications, and the measure of the impact that they have. At this time, CIHR is not able to report on the impacts of publications stemming from CIHR-related research. However, CIHR's Impact Assessment Team is currently working on identifying ways in which to capture such data.
As shown in Figure 3, the number of Canadian health research publications increased steadily from 1997 to 2005, peaking at about 17,000 publications in 20055. The increased funding available during the first four years of CIHR's existence (2000 to 2004) corresponds with a detectable increase in research output starting in 2003-2004 (most grants are three-to-four years in length and require approximately one year before results are published). The Canadian share of total health publications produced by the G-8 nations, which had been stable at about 4% between 1992 and 2000, started to rise in 2003 and exceeded 4.75% in 2005. It is projected that this rate may stabilize around the 4.75% level for 2006.
5. There may be a slight underestimation as the data excludes certain publications in psychology and health sciences
Figure 3: Number of Canadian Publications in Health Research and World Share6
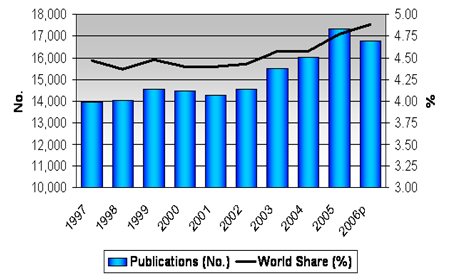
Source: Observatoire des sciences et des technologies (OST)
As shown in Figure 4 Canada's rate of scientific production in health research is strong compared to the United States and is comparable to that of the United Kingdom7. This indicates that Canada may be considered to be a global leader in the production of health-related research publications as compared with some of the leading producers of health R&D research (see also Figure 2).
6. '2006p' in this graph represents 'projected rate in 2006'
7. These figures cover the majority of health research publications, but omit certain relevant publications in psychology and health services.
Figure 4: Per Capita Output of Publications in Health Research for Select Countries, 2006
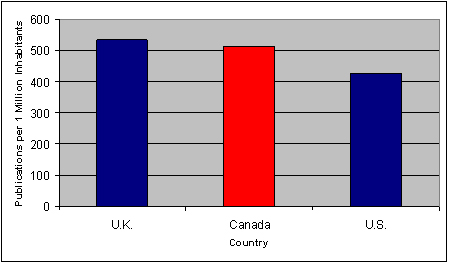
Source: Observatoire des sciences et des technologies, OECD, 2006 CIA World Fact Book.
3. Rating the quality of results of CIHR-funded research
A useful measure of the quality of research funded by CIHR is the degree to which resulting publications are cited (and in theory found useful). The citation impact for a group of researchers is the number of citations per paper that a group has received over a certain time period. A relative citation impact (RCI) can be calculated for any group of researchers and compared to an appropriate baseline. By this definition the RCI for the world is always 1.00 for any field and therefore if the RCI for Canadian researchers is greater than 1.00 then they are performing above the world average in that field.
As illustrated in Figure 5, the average relative citation factor for Canadian publications is approximately 1.1 when compared to the world average. This again, provides some indication that Canada's health research is favorably received, however, many other factors may contribute to variations on this measure such as: the types and substantive domains of research; the duration of the research (long-term vs. short-term R&D); and the overall "popularity" of various areas of research.
Figure 5: Average Relative Citation Factor (ARC) in Health Research, 20068
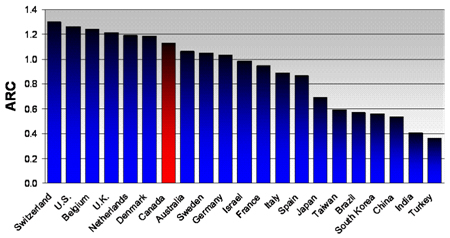
Source: Observatoire des sciences et des technologies (OST)
8. Only includes countries with at least 4,000 publications in health research in 2006 (excludes publications in psychology and health sciences).
Performance at the Program Activity Level of the MRRS
The following sections present the results achieved in 2007-2008 within each of the Program Activities that contribute to Strategic Outcome 1.0 - Outstanding Research.
Program Activity 1.1: Fund Health Research
CIHR supports the development of new knowledge through health research across all disciplines that are relevant to health. CIHR provides grants for both investigator-initiated research (also known as open research, due to the fact that researchers can choose the field of research they want to focus on) and strategic research (priority areas determined by CIHR's 13 Institutes) through competitions in conjunction with many partners.
Financial Resources ($M)
| Planned Spending | Authorities | Actual Spending |
|---|---|---|
| $493.5 | $535.7 | $539.5 |
Human Resources
| Planned | Actual | Difference |
|---|---|---|
| 230 | 204 | -26 |
|
Expected Results Effective and efficient funding programs that enable ethical health research creating health knowledge that responds to opportunities and priorities. |
Indicators
|
|
Link to Priority Priority #1: Research - Advance health knowledge, through excellent and ethical research, across disciplines, sectors and geography |
|
Program Activity 1.1 Performance Status: Successfully Met
The following presents a 2007-2008 performance summary of the key sub-activities that support the performance status of Program Activity 1.1 - Fund Health Research.
As outlined in more detail in the sections below, CIHR has successfully met the expected results for this program activity. This performance rating is based on assessment of planned and actual spending, activities and outputs. CIHR has supported the creation of new knowledge by making significant investments in health research across all disciplines that are relevant to health. Although there is limited data this year to support an evidence-based assessment of the success of the research programs, the level of application pressure for all of CIHR programs indicates that they are filling a need in the research community. The Institutes continue to influence the research agendas in their communities by funding a series of strategic initiatives in targeted areas.
A. Open Operating Grants Program (OGP)
The OGP represents CIHR's single largest investment. In 2007-2008, CIHR invested $380.2M, which represents 41% of CIHR's total
investment in grants and awards research. This open research support program encourages Canadian health researchers to pursue their very best ideas, define and pursue the mode of research best suited
to advance those ideas, and pursue the opportunities most likely to advance the impact of their work. Applications are accepted in all areas relevant to health and to CIHR's mandate
and are funded according to their excellence as determined by peer review. The health research capacity that this program helps to maintain is available to be mobilized when a national emergency (such
as SARS) threatens the health of all Canadians. As it is impossible to predict future health crises, it is necessary to maintain research capacity in all of the main fields of health, which this program
does.
In the 2007-2008 competition year, 3,626 applications were received (2,384 of these were deemed fundable) and 816 new projects were approved which means that only the top 23% of applications were approved for funding. The average project that is funded lasts 3-5 years so that in any given year the program funds approximately 3,500 new and ongoing projects. On average a new project receives $119,0009 per year. The number of projects supported by the OGP, together with program expenditures for the period 2000-2001 to 2007-2008 are shown in Figure 6 below.
9. Includes OGP grants in which the first year of payment is 2007-2008
Figure 6: Number of Projects Supported and Expenditures of the OGP
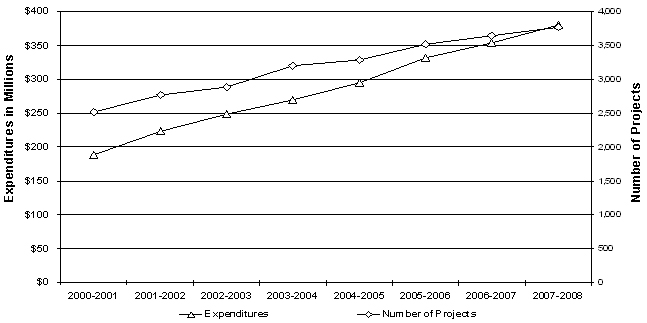
Source: CIHR Funding Database
Although more health research funding has become available to Canadian researchers, it has not necessarily become more accessible. Figure 7 shows the trends in the number of fundable10 applications to the OGP that were not funded, compared to the number funded, over the period of 2000-2001 to 2007-2008. As seen in Figure 7 approximately 1,500 high quality applications were left unfunded in the 2007-2008 Competition Year. Despite increases to the CIHR budget the funding rate for this program (which is the percentage of fundable applications that have been funded) has dropped significantly. In 2000-2001 CIHR was able to fund 58% of applications that were rated as worthy of funding through an expert review process, as of the 2007-2008 Competition Year, the funding rate has fallen to 34%. This is a slight increase over the 2006-2007 Competition Year (32%) and reflects a decrease in overall applications submitted to CIHR. This decrease may indicate a leveling-off of the application pressure to the OGP due to CIHR's communication of its intent to fund between 800 and 900 new grants per year in the OGP. This has established a reasonable expectation within the research community as to the level of support available and the competitiveness of this program. The high application pressure to the OGP program can be seen as measure of success since it is highly competitive and filling the needs of the research community.
10. CIHR has a rating scale of 0-4.9 for the peer review of funding applications, and only applications rated 3.5 and above are eligible for funding.
Figure 7: Fundable Applications to the Open Operating Grants Program
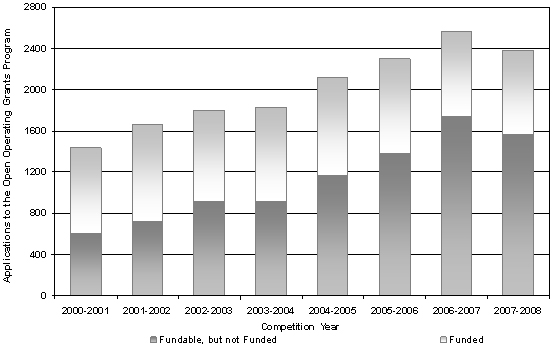
Source: CIHR Funding Database
Note: CIHR has a rating scale of 0-4.9 for peer review of funding applications, only applications rated 3.5 or higher are eligible for funding.
A study by the Council of Canadian Academies in 2006 found that in the health and life sciences, Canada is strong, relative to other countries, in a number of areas which happen to coincide with the areas that CIHR has been targeting. These include: cancer research and control; neuroscience; circulatory and respiratory health; infectious diseases and immunity; as well as emerging disciplinary fields such as: aboriginal health; aging; gender; and health. Much of the funding for these areas comes from the OGP.
The OGP was evaluated in 2004. Since the evaluation was completed, progress has been made in implementing the study recommendations. For example, the Research Reporting System was developed in 2007-2008 and will be implemented in 2008-2009 for the OGP competition; a new electronic newsletter targeted to researchers has been developed that identifies new developments regarding research funding; work is underway to improve the rating scale and criteria used by peer-review committees; and the success of entry-level applicants is being monitored.
Evidence that the OGP program is meeting expected results includes:
- The high application pressure to the OGP which has stimulated a large number of applications from many researchers in all areas of health research.
- Canada is strong in the health and life sciences relative to other countries in many areas being funded by CIHR in the judgment of both the Canadian Academy of Sciences and the Science, Technology and Innovation Council of Canada.
- The competitiveness of the program ensures that only the very best research is funded.
B. Team Grants
CIHR contributes funding to several team-related programs as part of its strategy to strengthen the research environment and enable outstanding research. In 2007-2008 a total of 26
teams were funded for up to five years through the open Team Grants competition. The average amount of funding per team in 2007-2008 was $739K. CIHR invested $19.2M in 2007-2008 on
the open Team Grant program. CIHR has found that many of the teams who have been successful under this "open" competition process are from research areas where there is already a strong
research capacity and infrastructure. As a result, this program is not adequately supporting research areas that are under-developed. An evaluation of the Team Grants, as well as other team type programs
is scheduled for 2008-2009.
C. Institute Strategic Initiatives
CIHR's broad-based approach brings together researchers across disciplinary and geographic boundaries through its 13 Institutes, each of which strategically addresses an area of health
research that is of importance to Canadians. The total expenditures of the Institute Strategic Initiatives that fall under this program activity were $31.7M in 2007-2008. In deciding how to allocate these
funds, the Scientific Directors of each of CIHR's 13 institutes and the Institute Advisory Boards are guided by the strategic plan of each Institute, as well as CIHR's
overall strategic plan (referred to as Blueprint) and discussions with other Institutes and external partners and decisions by CIHR's Research and Knowledge Translation Committee
(RKTC).11 Researchers are invited to submit research proposals to address the research priorities identified by the Institutes, which are then reviewed
through CIHR's expert peer review process.
11. Established in 2007 (prior to 2006-2007 this committee was called the Research Planning and Priorities Committee).
Table 4: Key Strategic Research Themes Funded by the Institutes in 2007-2008
| Institute | Key strategic research themes funded in 2007-2008 |
|---|---|
| Aboriginal Peoples' Health |
- Aboriginal Health Determinants |
| Aging |
- Mobility in Aging - Cognitive Impairment in Aging - Longitudinal Research Platform for Healthy and Successful Aging |
| Cancer Research |
- Access to Quality Cancer Care |
| Circulatory and Respiratory Health |
- Cardiovascular Complications of Diabetes |
| Gender and Health |
- Boys and Men's Health - Gender, Mental Health and Addictions |
| Genetics |
- Genes to Genomic Medicine - Health Services for Genetic Diseases - Genetics and Ethical, Legal and Social Issues |
| Health Services and Policy Research |
- Access to Appropriate Care across the Continuum - Drug Policy (Quality, Safety, and Financing) - Health Information |
| Human Development, Child and Youth Health |
- Indoor Air and Asthma / Allergy - Child Health Indicators |
| Infection and Immunity |
- HIV/AIDS - Emerging Infections and Microbial Resistance - Pandemic Influenza Preparedness - Vaccines of the 21st Century |
| Musculoskeletal Health and Arthritis |
- Physical Activity, Mobility and Health - Tissue Injury, Repair Replacement - Pain, Disability Chronic Diseases |
| Neurosciences, Mental Health and Addiction |
- Co-morbidity and Co-occurrence of Brain Disorders with other Health Problems - Research in Addiction - Mental Health in the Workforce |
| Nutrition, Metabolism and Diabetes |
- Obesity and Healthy Body Weight - Intervention Research on Healthy Living and Chronic Disease Prevention |
| Population and Public Health |
- Global Health - Impacts of the Social, Physical and Built Environments on Health - Understanding and Promoting Equity in Health |
The IRP concluded that "The Institutes have all achieved considerable progress in developing and implementing an agenda to coordinate and develop their research area... Despite resource constraints, these Institutes have operated extremely effectively. Each has developed a specific set of strategic initiatives as well as provided leadership through training initiatives, mentoring and workshops."12
D. Large Strategic Initiatives
CIHR's Strategic Plan, Blueprint, calls upon the organization to develop national research platforms and initiatives.
CIHR's Governing Council has identified a number of partnered, long-term strategic initiatives to pursue in order to address Canada's health research priorities. This program funds
large scale and long-term projects that cut across several health-related fields and that are too big for one Institute to fund alone. The topic areas are chosen by CIHR from its research
priorities on the basis of their potential for significant impact. As planned in the approved CIHR 5-Year Evaluation Schedule, an evaluation of CIHR's Large Strategic
Initiatives is scheduled for 2010-2011. A description of CIHR's Clinical Research Initiative is provided as an example of one of CIHR's eight Large Strategic Initiatives:
The Clinical Research Initiative (CRI) is CIHR's response to a clear need and opportunity to strengthen Canadian clinical research to accelerate the translation of clinical research discoveries into improved and cost-effective approaches to maintaining health and treating illness, and to provide evidence for sound health policies and an efficient health-care system. In 2007-2008 there was a total CIHR investment of over $14.3M towards the various programs offered through the CRI Initiative. One of the key programs launched in 2007-2008 is the CIHR/CFI Regional/National Clinical Research Initiatives with a major focus on building the excellence, national capacity and critical mass required to allow Canada to become an international leader in clinical research that leads to a better health-care system, improved health and a stronger economy. Under the CRI, through which funding starts in 2008-2009 the CFI and CIHR challenged institutions and their investigators to consider non-traditional models and/or combinations of traditional/non-traditional models to best meet the overall objective of enhancing clinical research through multidisciplinary and collaborative approaches. Integral components of the proposals included multidisciplinary research teams focused on high impact, clinically relevant health problems, training programs in clinical research, formal knowledge translation programs and a strong underlying ethics framework.
12. CIHR Year 5 International Review Panel Report 2000-2005, June 2006, p. 11. (http://www.cihr-irsc.gc.ca/e/31464.html)
|
Benefits to Canadians Vulnerable Populations - Children Poor children gain more weight Breastfed babies ace IQ tests Child abuse can alter biology |
E. Randomized Control Trials (RCT) Program
The RCT Program supports RCTs that provide rigorous evidence on the efficacy and effectiveness of interventions in health and health
services which make it well aligned to government priorities. The open program funded over 74 trials in 2007-2008 at a cost of $32.3M.
The RCT Program is seen to be very effective due to its strong applied focus and the numerous high impact Canadian trials that have been funded. However, the trials are longer, lasting up to ten years and more costly than open operating grants. The current average total investment for the duration of a new grant is $1.6M13. The high cost and long duration of RCTs make them difficult for CIHR to fund. The performance of this program can be improved by ensuring a more sustainable level of funding. CIHR is committed to increasing its funding for this program in 2008-2009. Increases will come from internal reallocations and future budgetary increases consistent with CIHR's five year investment plan.
13. Includes OGP grants in which the first year of payment is 2007-2008. Figures are to date as of May 2008 and are subject to change
F. HIV/AIDS Research Initiative
CIHR's HIV/AIDS Research Initiative is responsible for the management and oversight of the research components of the
two major Government of Canada initiatives in HIV/AIDS, namely: the Federal Initiative to Address HIV/AIDS in Canada (FI); and the Canadian
HIV Vaccine Initiative (CHVI). Through support via the FI (a partnership between the Public Health Agency of Canada (PHAC), Health Canada (HC), Correctional Service Canada, and CIHR) CIHR funds
research in the areas of: biomedical/clinical; health services and population health; community-based; and the Canadian HIV Trials Network. Through the new CHVI,
a partnership between the Government of Canada (PHAC, HC, Industry Canada, the Canadian International Development Agency, and CIHR) and the Bill & Melinda Gates Foundation,
CIHR funds research to accelerate the development of an HIV vaccine and address critical research gaps. With this combined funding, and further support from
CIHR, HIV/AIDS related research expenditures totalled approximately $37.1M in 2007-2008.
While research is a long-term endeavour, many of the funded projects have already demonstrated tangible outcomes. The HIV/AIDS Research Initiative is undertaking an evaluation of its HIV/AIDS Community Based Research Program (CBR) Program, which will be completed in spring 2009. The Canadian HIV Trials Network (CTN) was recently independently evaluated and the network scored highly in all areas reviewed. The evaluation noted that the CTN has played a key role in Canada's response to the HIV/AIDS epidemic and further funding will help ensure continued Canadian strength and expertise in conducting important and high quality clinical trials in HIV.
|
Benefits to Canadians - HIV/AIDS Discoveries Male circumcision Natural gene can shut down HIV Protein protection from killer diseases |
Risks and Challenges - Strategic Outcome 1.0
When delivering results in 2007-2008 related to Strategic Outcome 1.0 - Outstanding Research, CIHR proactively managed the following risks:
Risk # 1: Managing complexity of long-term investment mechanisms: There is a risk that funding via an annual appropriation may make it difficult for CIHR to provide longer term funding mechanisms that vary throughout the lifecycle of a research project. This may limit CIHR's ability to initiate new programs that meet the temporal needs of the researcher community.
Impact: Research takes time and a sustained investment. It is also subject to considerable uncertainty. A large portion of CIHR's budget is committed to grants and awards that extend over three to five years. In many cases small levels of investment in the first years of a project results in larger commitments in the third and fourth years although the actual spending profile itself is often not predictable. Not managing the complexity of these funding mechanisms results in limited flexibility for new investments which could reduce CIHR's ability to address specific health challenges as they arise.
Mitigation: To mitigate this risk CIHR is in the process of implementing a five year investment roadmap for the grants and awards budget which is supported by more sophisticated investment modelling processes. This allows the organization to better forecast the future impacts of funding decisions and to implement concepts of "steady-state" dynamics to ensure relative stability of investments over time.
Risk # 2: Ensuring organizational capacity to address Strategic Priorities: There is a risk that CIHR may not have the agility and flexibility required to quickly address strategic priorities in targeted areas.
Impact: There is an increasing requirement to ensure that health research knowledge is developed in targeted areas to address specific issues and concerns and respond to government priorities. This typically occurs because there is a gap in the current knowledge base and/or a requirement to strengthen and expand the existing knowledge base to respond to a significant health challenge. If CIHR does not have the organizational capacity to respond to priorities it could result in specific health challenges not being addressed.
Mitigation: The Institute structure and the Advisory Boards that support them allows CIHR to mitigate this risk by keeping abreast of the critical health challenges that need to be addressed and the research capacity that exists in Canada to address these challenges. Each Institute is led by a Scientific Director who plays a leadership role in his/her area of expertise and attempts to anticipate future requirements through the development of strategic plans.
Risk # 3: Ability to recruit peer reviewers: There is a risk that CIHR may be unable to continue to recruit highly qualified peer reviewers to evaluate research proposals.
Impact: The peer review process is a critical component of the delivery of CIHR programs. This process ensures fairness and transparency, good value for money, and that the best and brightest researchers are funded. The inability to recruit new peer reviewers results in fatigue for the reviewers that remain, reliance on less experienced reviewers, inferior reviews and delays in the overall peer review process.
Mitigation: To mitigate this risk CIHR has established a central group to coordinate the peer review process including the recruitment of peer reviewers. This group is also in the process of identifying ways to streamline and improve the peer review processes to reduce the burden on peer reviewers.
Strategic Outcome 2.0: Outstanding Researchers in Innovative Environments
Strategic Outcome 2.0 focuses on building a:
Strong health research community able to undertake outstanding research.
Developing a community of outstanding health researchers is another part of CIHR's core business. The main instruments used by CIHR to develop health research capacity in Canada are training and salary awards, Institute-led partnerships and ethical research standards.
Summary of Results
CIHR uses several indicators to monitor long-term trends in this area, two such indicators being:
- Percent of PhD graduates in Canada planning postdoctoral studies in health; and
- Quality and availability of adequate resources for research (e.g., infrastructure, hardware and software).
Indicators at the strategic outcome level are general societal indicators. CIHR contributes to the development of highly qualified personnel (HQP) through direct investments in people via training and salary awards and indirectly through grants as many trainees are involved in CIHR Operating grants.
1. Percent of PhD graduates in Canada planning postdoctoral studies in health
The percentage of PhD graduates planning postdoctoral work is a key indicator of both the likelihood of PhD training encouraging individuals to continue in health research, as well as the potential demand for CIHR postdoctoral fellowship awards. According to the 2005 Survey of Earned Doctorates, 56% of all graduates planned to enter the labor force after graduation, while 34% were planning to undertake a postdoctoral fellowship.14 However, for those graduating in the life sciences, approximately 64% were planning on continuing their training or study through a postdoctoral fellowship or other arrangement. These data support the concept that the majority of PhD graduates in areas of health/medical research are motivated to continue conducting research in their field after they have completed their academic training. The findings also validate CIHR's increased emphasis on encouraging students and trainees to complete their graduate degrees through fellowships, scholarships, grants and awards.
2. Quality and availability of adequate resources for research
The 2005 survey of CIHR-funded researchers found that 70% agreed that the environmental capacity (e.g., infrastructure, hardware and software) to sustain researchers in conducting their research, is reasonably adequate or optimal, with 8% saying that their research environment is to a large extent optimal. As Figure 8 demonstrates, researchers connected to CIHR Institutes clearly identify capacity building as an area of high need; ranging from 88% for the Institute of Health Services and Policy Research (IHSPR) to 70% for the Institute of Genetics (IG).
14. Data taken from Gluszynski, Tomasz and Valerie Peters, Survey of Earned Doctorates: A Profile of Doctoral Degree Recipients, Statistics Canada and Human Resources Development Canada, 2005, p. 14.
Figure 8: Need for Institutes to Develop Capacity - Funded Researchers
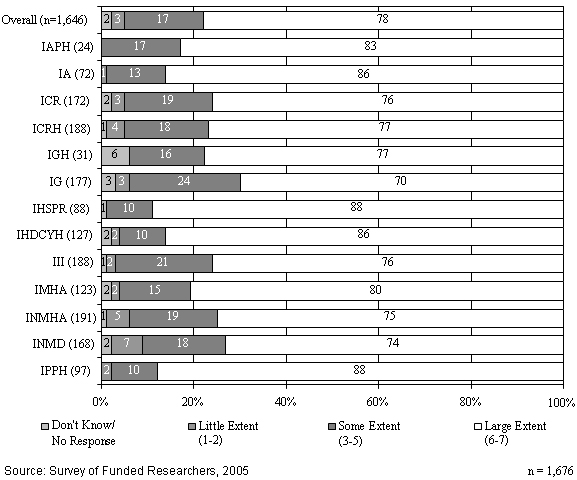
Performance at the Program Activity Level of the MRRS
The following sections present the results achieved in 2007-2008 within each of the Program Activities that contribute to Strategic Outcome 2.0 - Outstanding Researchers in Innovative Environments.
Program Activity 2.1: Fund Health Researchers and Trainees
One of CIHR's core objectives is to provide leadership in building capacity within Canada's health research community. This is done through the training and development of researchers, and by fostering the development and ongoing support of scientific careers in health research. In addition to providing trainees and independent investigators with salary support, CIHR is committed to helping them develop the skills they require to succeed in the modern research environment.
Financial Resources ($M)
| Planned Spending | Authorities | Actual Spending |
|---|---|---|
| $203.6 | $208.5 | $202.3 |
Human Resources
| Planned | Actual | Difference |
|---|---|---|
| 95 | 84 | -11 |
|
Expected Results Effective and efficient funding programs that ensure a supply of highly trained health researchers and trainees are available to conduct outstanding research. |
Indicators
|
|
Link to Priority |
|
Program Activity 2.1 Performance Status: Successfully Met
The following presents a 2007-2008 performance summary of the key sub-activities that support the performance status of Program Activity 2.1 - Fund Health Researchers and Trainees.
As outlined in more detail in the sections below, CIHR has successfully met the expected results for this program activity of ensuring that a supply of highly qualified personnel (HQP) is available to conduct outstanding research. This performance rating is based primarily on an assessment of planned and actual spending, activities and outputs. CIHR has made significant investments in supporting health researchers and has increased the research capacity within all disciplines that are relevant to health. Although there is limited data this year to support an evidence-based assessment of the success of these programs anecdotal evidence such as the level of application pressure indicates that they are filling a need in the research community. Furthermore significant budget increases through Budget 2007 to the Canada Research Chairs Program and the Canada Graduate Scholarships Program indicate the continued success and relevance of these programs in supporting Canada's health researchers. The Institutes continue to build capacity in their communities by funding a series of strategic training and salary awards in targeted areas.
A key instrument used by CIHR to develop health research capacity in Canada is training and salary awards. CIHR supports training and salary in two streams: open training and salary support, which is not targeted; and strategic training and salary support, which is targeted to priority research areas identified by the 13 Institutes. Other activities include CIHR's participation in the Canada Research Chairs and Canada Graduate Scholarships programs.
A. Training Awards
CIHR's training awards support more than 2,400 individuals, including undergraduates, masters and doctoral students, and postdoctoral fellows. Expenditures incurred for the training
support programs in 2007-2008 were $51.9M.
The open training programs have three main components:
- Doctoral Research Awards (DRAs);
- Strategic Training Initiative in Health Research (STIHR); and
- Fellowships
The STIHR program was evaluated in 2007-2008 to provide evidence on program performance, to facilitate corporate decision-making around program renewal and funding decisions, and to fulfill reporting requirements to central agencies. Based on the key findings, it was recommended that CIHR review and revise the level of funding for the open STIHR program. CIHR plans to address this observation by better aligning its STIHR program to strategic priority areas rather than open research. The final report is expected to be publicly available by September 2008.
A recent evaluation of the STIHR program concluded that it has performed as well as programs like the Canada Graduate Scholarships, the Doctoral Research Awards, and CIHR Fellowship awards in terms of trainees' disciplinary background; early scholarly productivity; and perceptions of the training environment and trainee experience. Additionally, the program appeared to be increasing the number of research training opportunities for health systems and services and clinical trainees.
Figure 9 shows the number of people in health research across Canada who were supported by various CIHR awards programs in 2007-2008.
Figure 9: Research Capacity Building Support in 2007-2008
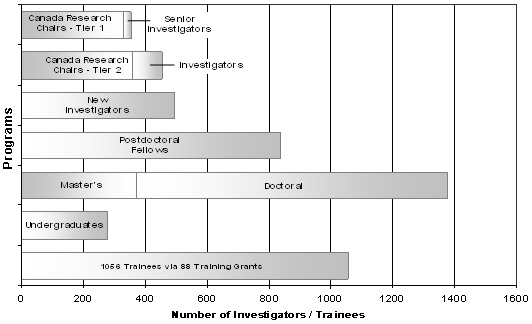
Source: CIHR Funding Database
B. Salary Support Programs
Under the Salary Support Programs, approximately 60 New Investigators start their funding each year through the open competition. In a few years the programs should reach a steady state, where
a total of approximately 300 new investigators will be supported at any given time. This funding enables them to focus a minimum of 75% of their time on research (rather than teaching, administration
or clinical work).
As seen in Figure 10, expenditures incurred for the CIHR Salary Support Programs declined in 2007-2008 to approximately $30.7M as compared to approximately $32M in 2006-2007. This trend is expected to continue in the 2008-2009 fiscal year, due to the termination of the Investigator, Senior Investigator and Distinguished Investigator programs. Salary awards are also being terminated early due to the uptake of Canada Research Chairs by recipients of CIHR salary awards (as per CIHR regulations, an individual may not hold a CIHR salary award and a Canada Research Chair concurrently).
Figure 10: Expenditures in Training and Salary Support
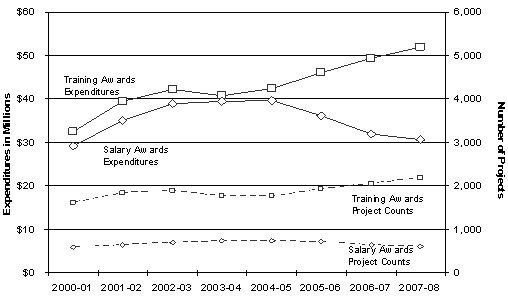
Source: CIHR Funding Database
Note: Salary Award figures exclude the Canada Research Chairs
C. Strategic Training and Salary Support Programs - Role of CIHR's 13 Institutes
A key role of CIHR's Institutes is building capacity through training and salary support in strategic health research areas identified by the Institutes in consultation with stakeholders
from government, health-care organization, patient groups, and industry. The Strategic Training and Salary Support Programs provide support and special recognition primarily to students who are pursuing
a master's or PhD degree, or for highly qualified candidates at the postdoctoral or post-health professional degree stages. The 13 Institutes provide training
support through a number of mechanisms, including:
- Strategic Training Initiative in Health Research (STIHR);
- Priority Announcements; and
- CADRE Program of targeted post-doctoral fellowships.
In addition to those mentioned above the Institutes build capacity through their own strategic initiatives. One such example includes the following:
As one of its first initiatives, the CIHR-Institute of Aboriginal Peoples' Health (IAPH) established the Aboriginal Capacity and Developmental Research Environments (ACADRE) centres to develop a network of supportive research environments across Canada to facilitate the development of Aboriginal capacity in health research. The centres are dedicated to improving First Nations, Inuit and M�tis peoples' health through community-based and scientifically excellent research. The performance of these centres was seen as successful as all ACADREs made marked progress towards achieving the program's overall goals. With the aim to sustain and ensure momentum of the ACADRE centres, CIHR-IAPH launched a new initiative and funding commenced in the fall of 2007 for the second phase of the program with the Network Environments for Aboriginal Health Research (NEAHR). The federal government demonstrated support for this program in early 2008 when Parliamentary Secretary Steven Fletcher announced an investment in the NEAHR program of $15.8M over the next three years.
D. Canada Research Chairs (CRC)
The Canada Research Chairs Program invested approximately $315M in 2007-2008 to attract and retain some of the world's most accomplished and promising minds. CIHR expenditures for the
CRC Program have grown significantly over the past few years, from $72.9M in 2005-2006 to approximately $86.5M in 2007-2008. CIHR planned spending and expenditures
for the CRC Program have increased each year since 2005-2006 due to incremental increases received by CIHR for the Program. CIHR lapsed significant
funds for the CRC Program in each fiscal year (2005-2006 through 2007-2008) due to difficulties encountered by the universities in filling the Chairs.
As of November 2007, there were a total of 1,851 active Chairs. More than 2,000 researchers have held CRCs since the beginning of the program. Therefore, the program has met its goal of supporting 2,000 chairholders by the end of 2008, in spite of lapsing funds over the last three years. The fifth-year evaluation of the program concluded that the CRC Program has helped to create a research environment that is conducive to the long-term retention and attraction of top researchers. Chairholders reported significant increases in research productivity and number of HQP being trained at the graduate level since receiving their Chair awards compared to other researchers over the same time period. Also, they reported research impacts such as patents, inventions and potential health treatments which can be at least partly attributable to the CRC Program.
E. Canada Graduate Scholarships (CGS)
The CGS Program provides financial support to develop future researchers at both the master's and doctoral levels, providing them with an opportunity to gain research experience. In
2007-2008 CIHR invested $13.9M in the CGS Program. In its 2007 Budget, the Federal Government announced new funding for CIHR's CGS
Program to enable CIHR to fund an additional 400 scholarships on an ongoing basis by the time the program is fully implemented in 2009-2010.
The CGS Program is currently undergoing a joint evaluation with SSHRC and NSERC. CIHR is the lead on this Tri-agency evaluation for which the final report will be ready in late 2008.
Program Activity 2.2: Fund Research Resources, Collaboration and other Grants to Strengthen the Health Research Community
CIHR is strengthening the health research community's ability to conduct research by supporting research-enabling activities and resources. This includes supporting large teams of researchers from across disciplines in resolving some of the most complex health problems facing Canadians, engaging in collaborative activities such as networking and providing and maintaining state-of-the-art tools such as new equipment, databases and other specialized resources to conduct research.
Financial Resources ($M)
| Planned Spending | Authorities | Actual Spending |
|---|---|---|
| $70.0 | $69.7 | $68.0 |
Human Resources
| Planned | Actual | Difference |
|---|---|---|
| 33 | 29 | -4 |
|
Expected Results Effective and efficient partnerships and funding programs that lead to a dynamic research environment and outstanding research. |
Indicators
|
|
Link to Priority Priority #2 - Researchers - Develop and sustain Canada's health researchers in vibrant, innovative and stable research environments. |
|
Program Activity 2.2 Performance Status: Successfully Met
The following presents a 2007-2008 performance summary of the key sub-activities that support the performance status of Program Activity 2.2 - Fund Research Resources, Collaboration and other Grants to Strengthen the Health Research Community.
As outlined in more detail in the sections below, CIHR has successfully met the expected results for this program activity of effective and efficient partnerships and funding programs that lead to a dynamic research environment and outstanding research. This performance rating is based primarily on an assessment of planned and actual spending, activities and outputs. In 2007-2008 CIHR strengthened the health research community's ability to conduct research by providing funds to acquire the necessary resources required to conduct research. The Institutes played a key role by funding various team grants within their respective research communities.
A. Institute-strategic Team Grants
The majority of expenses under this program activity arise from New Emerging Team grants (NETs) and Interdisciplinary Capacity Enhancement team grants (ICEs) funded through the institutes and other CIHR strategic initiatives. In 2007-2008 CIHR funded 124
NETs representing approximately $30.1M and 45 ICEs representing approximately $7.4M.
An evaluation of all of CIHR's Team-Type Programs (numbering approximately ten) is being initiated in 2008-2009 and is expected to report in 2010 on the relative success and limitations of those programs.
In this context, an additional benefit is that some of the work of this evaluation will result in contributions to the development of tools for measuring knowledge translation and capacity enhancement in the CIHR and Canadian Research environment. The design of the Team-Type programs will be examined in the light of Team science and what is needed to establish increasingly productive and innovative teams (or team-type funding programs). This could be an exceptional opportunity for management to review CIHR's Team-Type Programs and to align their requirements and funding with known factors of Team science success.
B. Research Resources and Collaboration Program (RRC)
The RRC Program is made up of a number of sub-programs, all with the goal of strengthening the health research community's ability to conduct research. CIHR expenditures
for the RRC Program totalled approximately $6.8M in 2007-2008. The decline in expenditures is due primarily to the fact that the Research Resource Grant program has not been re-launched
since 2005.
|
Benefits to Canadians - Advances in Neuroscience Adult neural stem cells Neuroscience: |
C. Regional Partnerships Program (RPP)
This program helps build partnerships and is designed to enable researchers in less populous and less economically prosperous regions of Canada. The program provided 94 grants and 50 awards to researchers
and trainees (combined amount of new and ongoing grants and awards) in 2007-2008. The total CIHR funds paid out in the fiscal year 2007-2008 totaled $4.4M. The CIHR
funding for grants and awards is matched by partners to a ratio of 1:1. An evaluation of the RPP in 2005 recommended a redesign to ensure that activities would better meet expected
results. This redesign has since taken place with extensive input from key stakeholders. The RPP is the sole CIHR program focused on the development of health research
capacity in lower resourced regions. It is very positively rated by participating researchers, Advisory Committee members, and other stakeholders.
Program Activity 2.3: Develop and Support a Strong Health Research Community Through National and International Alliances and Priority Setting
CIHR is developing strong national and international partnerships through its 13 Institutes to advance strategic health research priorities and leverage funding and expertise for research. These partners include health policy makers at provincial, federal, and international levels of government, the private sector and voluntary health organizations from Canada and abroad.
Financial Resources ($M)
| Planned Spending | Authorities | Actual Spending |
|---|---|---|
| $28.1 | $28.2 | $24.0 |
Human Resources
| Planned | Actual | Difference |
|---|---|---|
| 13 | 12 | -1 |
|
Expected Results National and international health research agendas as well as strong alliances and partnerships are formulated and implemented. |
Indicators
|
|
Link to Priority Priority #2 - Researchers - Develop and sustain Canada's health researchers in vibrant, innovative and stable research environments. |
|
Program Activity 2.3 Performance Status: Successfully Met
The following presents a 2007-2008 performance summary of the key sub-activities that support the performance status of Program Activity 2.3 - Develop and Support a Strong Health Research Community through National and International Alliances and Priority Setting.
As outlined in more detail in the sections below, CIHR has successfully met the expected results for this program activity of implementing and formulating national and international health research agendas as well as strong alliances and partnerships. This performance rating is based primarily on an assessment of planned and actual spending, activities and outputs. In 2007-2008 CIHR continued to collaborate with hundreds of its partners including the Tri-agencies, non-profit, national and international organizations and has leveraged significant funding to maximize its investment in health research and to facilitate the knowledge exchange and translation of research results. Although there is limited data this year to support an evidence-based assessment of the success of these programs the number of partnerships and the amount of funding leveraged by these partnerships substantiate the rating of 'successfully met'. The Institutes play a crucial role in creating and building partnerships across all disciplines of health research.
A. Institute Support Grants (ISG)
The Institute Support Grants (ISG) Program provides $1.0M to each of CIHR's 13 Institutes for its operational, strategic
and development activities. A management review of the ISG Program undertaken in 2007-2008 concluded that alternative models would not meet the required elements of the virtual Institute
model and demonstrated that the ISG Program is deemed to be the most appropriate, efficient and cost effective funding mechanism for the Institutes.
B. Small Health Organizations Partnership Program (SHOPP)
This program increases the research funding capacity of health charities and non-profit organizations. The program provides nearly 60 awards (combined amount of new and existing awards in 2007-2008) to
trainees. The total CIHR funds paid out in 2007-2008 totalled over $800K. The findings of the 2007 evaluation of SHOPP indicated that the program is having a significant
positive impact on the research community.
C. Human Frontier Science Program (HFSP)
This program provides grants to support intercontinental collaboration in basic research at the frontier of human knowledge of biology. It also emphasizes support for young researchers by offering post-doctoral
fellowships that support outstanding candidates. A recent expert panel review of the HFSP showed it is meeting its objectives of promoting interdisciplinary and new collaborations,
and is filling a unique niche in international research funding.
|
Benefits to Canadians - Aboriginal Peoples Inuit obesity in step with Euro-Canadian rates CIHR sets guidelines for Aboriginal studies Researchers tackle tooth decay epidemic among Aboriginal children |
Program Activity 2.4: Inform Research, Clinical Practice and Public Policy on Ethical, Legal and Social Issues (ELSI) Related to Health and Health Research
CIHR funds research on ethical, legal and social issues (ELSI) related to health and health research and strives to build capacity in Canada in the field of research ethics. The ELSI program is related to all other CIHR programs, as its legislation requires that it promote or fund research that "meets the highest international scientific standards of excellence and ethics".
Financial Resources ($M)
| Planned Spending | Authorities | Actual Spending |
|---|---|---|
| $6.3 | $6.3 | $2.2 |
Human Resources
| Planned | Actual | Difference |
|---|---|---|
| 3 | 3 | 0 |
|
Expected Results Uptake and application of ethics knowledge as an integral part of decision-making in health practice, research and policy. |
Indicators
|
|
Link to Priority Priority #2 - Researchers - Develop and sustain Canada's health researchers in vibrant, innovative and stable research environments. |
|
Program Activity 2.4 Performance Status: Not Met
The following presents a 2007-2008 performance summary of the key sub-activities that support the performance status of Program Activity 2.4 - Inform research, Clinical Practice and Public Policy on Ethical, Legal and Social Issues (ELSI) Related to Health and Health Research.
As outlined in more detail in the sections below, CIHR has not met the expected results for this program activity of increasing the uptake and application of ethics knowledge as an integral part of decision-making in health practice, research and policy. This performance rating is based on an assessment of planned and actual spending, activities and outputs. In 2007-2008 due to the underutilization of the funding for this program activity, a management decision was made to reduce the planned spending amount and reallocate these funds to other programs. CIHR had over estimated the capacity of the health research community to undertake studies into health research ethics. As a result, the actual spending for this activity was significantly less than then planned amount identified in CIHR's 2007-2008 Report on Plans and Priorities. As a result the decreased investment, the reach of the program was less than anticipated. It should be noted, however, that this change in planned spending does not change CIHR's commitment to ensure that all CIHR funded research is conducted in an ethical manner.
A. Ethical, Legal and Social Issues (ELSI)
The standards for ethics research developed and administered under this program are recognized as the gold standard in Canada and have been incorporated into the rules of all major institutions. In 2007-2008,
CIHR invested approximately $1.8M to support ELSI-related grants and awards. Notwithstanding these efforts, a portion of the allocated funding has been consistently
underutilized. CIHR intends to continue its efforts at building receptor capacity to conduct research into ethics and is confident that over time this issue will be addressed.
Despite these challenges, the ELSI Program has had some great accomplishments in 2007-2008, including the publication of Guidelines for Health Research Involving Aboriginal People, developed by CIHR at a time when no government agency had a clear mandate in this highly sensitive area. The guidelines can be found on CIHR's website at the following address: http://www.cihr-irsc.gc.ca/e/29339.html.
|
Benefits to Canadians - Environment and Health Once-common contaminants linked to lymphoma Does pollution hit women harder? The Ontario Medical Association estimates that 1,900 Ontarians die prematurely each year from ambient air pollution exposure, and that the economic costs of these and other health effects total more than $1 billion per year. A CIHR-funded study is the first in North America to draw a link between Parkinson's disease and manganese air pollution, and suggests that industry-generated emissions of the pollutant pose a greater health risk than traffic-generated manganese. "This study of 110,000 people over three years supports the theory that exposure to manganese adds to the natural loss of neurons attributable to the aging process," says Dr. Murray Finkelstein at the University of Toronto, one of the study's authors. The results appear in a recent issue of Environmental Research. |
Risks and Challenges - Strategic Outcome 2.0
In delivering results in 2007-2008 related to Strategic Outcome 2.0, Outstanding Researchers in Innovative Environments, CIHR proactively managed the following risks:
Risk # 1: Canada's potential future research personnel shortage: There is a risk that Canada may face shortages in research personnel in the future.
Impact: Given the increasing demand for high-quality researchers around the world at a time of increasing rates of retirement among senior researchers, a shortage of personnel conducting research on new health products and services could place Canadian economic competitiveness at risk. This issue was identified in a 2007 Conference Board of Canada report card that assessed Canada's socio-economic performance. The report noted that: "Canada has a shortage of the skilled people who are essential for innovation. We have 7.2 researchers per 1,000 employees, compared with 16.5 per 1,000 in top-ranked Finland. Canada ranks 12th among the 17 comparator countries in the proportion of graduates with science and technology degrees"15. The impact of not adequately addressing this challenge is that Canada may lack the intellectual capital to conduct the research needed to support improvements in the health of Canadians and the health-care system.
Mitigation: This risk is being mitigated by making research capacity development a priority and funding both individual awards and strategic health research training programs to address capacity gaps. The expanded Canada Graduate Scholarships program, the new Vanier Scholarships and the Canada Research Chairs program will help attract and retain researchers.
15. Conference Board of Canada, How Canada Performs: A Report Card on Canada, June 2007, available at: http://www.conferenceboard.ca/documents.asp?rnext=2047
Risk # 2: Ensuring alignment of programming with other granting agencies: There is a risk that CIHR's programming overlaps with programs already in place in other granting organizations.
Impact: This could result in over-investing in certain areas with limited resources available in other areas of need.
Mitigation: To mitigate this risk, CIHR makes a concerted effort to work with other federal funding agencies - the Natural Sciences and Engineering Research Council (NSERC) and the Social Sciences and Humanities Research Council (SSHRC) to create inter-agency mechanisms that foster a more comprehensive approach to the overall management of research support. CIHR has established mechanisms for ongoing planning and exchange, the harmonization of policies and practices, and the collaborative delivery of programs.
Risk # 3: Effectiveness of partner selection and engagement: There is a risk that CIHR's approach to selecting and working with partners is ineffective and does not yield the types of partnerships required to have an impact on health research.
Impact: This could result in inconsistent and multiple contacts with the same partners, a large number of partner relationships to manage, missed opportunities and potentially partners choosing to stop working with CIHR.
Mitigation: To mitigate this risk CIHR has established a Partnership and Citizen Engagement Branch to ensure the consistent, coordinated and effective management of partnerships and citizen engagement activities across CIHR. CIHR is also in the process of developing a partnership strategy for CIHR which clearly outlines what the organization is trying to achieve through its partnerships. This strategy will identify the types of partnerships CIHR should be engaging with from all sectors, the key stakeholders CIHR should be engaging with and the anticipated outcomes of these relationships.
Strategic Outcome 3.0: Transforming Health Research into Action
Strategic Outcome 3.0 focuses on ensuring that:
Health research is adopted into practice, programs and policies for improved health of Canadians and a productive health system; stimulation of economic development through discovery and innovation.
A key part of CIHR's mandate, knowledge translation (KT) is a dynamic and iterative process that includes synthesis, dissemination, exchange and the ethically sound application of knowledge to improve the health of Canadians, provide more effective health services and products and strengthen the health care system. This is accomplished through the funding of KT research and activities; facilitation and management of partnerships that can accelerate KT; and the development of measurement, analysis and evaluation policies, frameworks and tools to assess the outcomes and impacts of CIHR-funded research. CIHR's KT strategy aims to accelerate the transformation of research results into health benefits for Canadians and an improved health-care system. CIHR also plays a role in helping to move promising new research breakthroughs toward potential commercial applications. Throughout 2007-2008, CIHR worked towards fulfilling the knowledge translation part of its mandate through targeted funding opportunities, the development of policies to facilitate KT and by expanding CIHR's messaging about KT within and outside of the organization.
Summary of Results
Several key strategic outcome indicators are used to monitor CIHR's progress in this area, including the following:
- Extent to which CIHR-funded researchers are integrating KT targets into their work; and
- Number of patents, spin-off companies and licenses for intellectual property generated from CIHR-funded research.
1. Extent to which CIHR-funded researchers are integrating KT targets into their work.
CIHR's policy on Access to Research Outputs took effect January 1, 2008 and applies to all grants funded after that date. Grant recipients must now make every effort to ensure that their peer-reviewed research articles are freely available as soon as possible after publication. Open access enables authors to reach a much broader audience, which has the potential to expedite awareness of and facilitate the use of research findings by policy makers, health care administrators, clinicians, and the public, by greatly increasing ease of access to research. CIHR funds several programs that require knowledge users within the health system decision makers as project team members, such as the Partnerships for Health System Improvement initiative. In 2007-2008, CIHR invested approximately $1.7M in this program, an amount that was matched at least one to one through partner contributions. KT plans are required and assessed as part of the application process to ensure that project findings are disseminated and applied to improve health-care in Canada. The Knowledge to Action and Knowledge Synthesis funding opportunities (discussed in more detail in section 3.1) also require knowledge users as part of the research team. These integrated KT funding opportunities require a collaborative or participatory approach to research that is action oriented and is solutions and impact-focused. Health research is adopted into practice by engaging the knowledge-user partner in defining the research question and in interpreting and applying the findings.
2. Number of patents, spin-off companies and licenses for intellectual property generated from CIHR-funded research
Health research leads to new products, companies and jobs. Data available for the past 10 years shows that 187 spin-off companies have been created by CIHR funded researchers, the majority of which are still active. Figure 11 illustrates the total number of health patents that have been issued each year, and how many of those patents are held by CIHR-funded researchers. The drop in the number of patents from 2006 to 2007 is of concern and requires further analysis to determine its causes and ramifications. CIHR is currently developing a KT Advisory Committee on Commercialization with the view of convening expert advice on how to best deploy our available resources in this area.
Figure 11: Number of Health Related Patents by Year
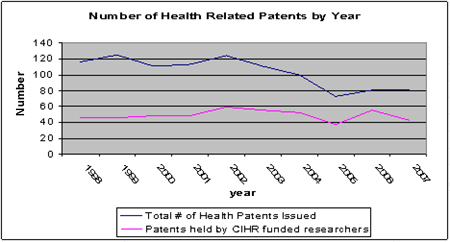
Source: US Patent Office Database
Figure 12 summarizes the grants and awards expenditures made by CIHR under Strategic Outcome 3.0 - Transforming Health Research into Action. Expenditures have grown substantially over the last six years, from $32M in 2000-2001 to $134M in 2007-2008. In 2007-2008 CIHR was allotted $73.5M for the Centres of Excellence for Commercialization and Research (CECR) program (see section 3.2). The Institutes have strongly supported KT research through their strategic initiatives.
Figure 12: CIHR Investments in the Knowledge Translation Mandate (transforming Health Research into Action
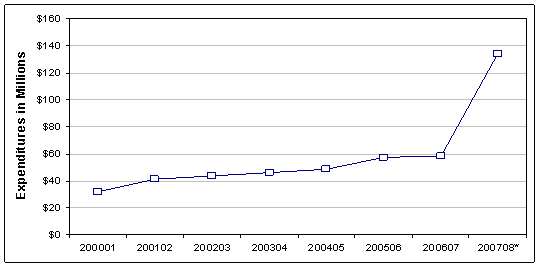
*In 2007-2008, $73.5M was funded through the Centres of Excellence for Commercialization and Research (CECR) program.
Source: CIHR Funding Database
Note: Includes the Networks of Centres of Excellence Program.
Performance at the Program Activity Level of the MRRS
The following sections present the results achieved in 2007-2008 within each of the Program Activities that contribute to Strategic Outcome 3.0 - Transforming Health Research into Action
Program Activity 3.1: Support Activities on Knowledge Translation, Exchange, Use and Strategies to Strengthen the Health System
A key part of CIHR's mandate, knowledge translation (KT) is about moving knowledge into action: turning the knowledge gained through health research into improved health for Canadians, more effective services and products, and a strengthened health system. CIHR's KT Strategy is designed to further expand and increase its ongoing efforts in this area. The strategy is a multi-year plan based on Blueprint that identifies planned activities in the following four areas: supporting research on KT concepts and processes; contributing to building networks of researchers and knowledge-users; improving the capability to support KT research focused on the synthesis of knowledge at CIHR and with partners; and supporting and recognizing KT excellence.
Financial Resources ($M)
| Planned Spending | Authorities | Actual Spending |
|---|---|---|
| $40.7 | $41.9 | $39.8 |
Human Resources
| Planned | Actual | Difference |
|---|---|---|
| 19 | 17 | -2 |
|
Expected Results Effective dissemination, exchange, synthesis and application of research results take place to create new knowledge, strengthen Canadian capacity and networks and, together with our partners, enable effective research and application of health research results. |
Indicators
|
|
Link to Priority Priority #3: Knowledge Translation - Catalyze health innovation in order to strengthen health and the health-care system and contribute to the growth of Canada's economy |
|
Program Activity 3.1 Performance Status: Successfully Met
The following presents a 2007-2008 performance summary of the key sub-activities that support the performance status of Program Activity 3.1 - Support Activities on Knowledge Translation, Exchange, Use and Strategies to Strengthen the Health System.
As outlined in more detail in the sections below, CIHR has successfully met the expected results for this program activity of the effective dissemination, exchange, synthesis and application of research results to create new knowledge, strengthen Canadian capacity and networks and, with partners, enable effective research and application of health research results. This performance rating is based primarily on an assessment of planned and actual spending, activities and outputs. The expected results have been achieved through increased funding for the Networks of Centres of Excellence program and increased focus on building and strengthening teams of researchers engaged in KT. The Institutes play an instrumental role in helping to achieve CIHR's KT mandate. CIHR's knowledge translation sub-programs are all relatively new (2-3 years old) and therefore an evidence-based assessment of their performance is not yet available. However, increasing application pressure indicates progress in building capacity in this area. CIHR is committed to significantly increasing its expenditures in knowledge translation activities.
A. Networks of Centres of Excellence (NCEs)
The NCE Program is a joint program with the three federal research councils in collaboration with Industry Canada. The NCEs
are unique partnerships among universities, industry, government and not-for-profit organizations resulting in the transfer of knowledge and exploitation of leading-edge research results with economic
or societal benefits to Canadians. During the period of 2001-2007, the program produced: 27,000 refereed publications; filed 720 Patents and issued 240; 140 Copyrights over 3,100 graduate students trained;
400 licenses granted or in negotiation; and 58 spin-off companies (over 120 spin-offs since the beginning of the program).
The report released in 2006 by the Council of Canadian Academies, The State of Science and Technology in Canada which can be found at this link: http://www.scienceadvice.ca/documents/The_State_of_Science_and_Technology_in_Canada.pdf, ranked the NCE Program as second for its support to commercialization, thanks to the partnerships it has nurtured with outside organizations and for its support in creating spin-off companies. The survey also included a summary of international reports on S&T that indicated the NCE Program's collaborations and networking efforts also have gained international recognition. In 2007-2008, an international advisory committee reviewed the NCE Program. The international review was favourable. Full details of the NCE's International Advisory Committee report can be found at the following address: http://www.nce.gc.ca/pubs/reports/2007/nce-iacreport/nce-iac-content_e.htm.
As well in 2007, the NCE program was evaluated under the guidance of an interagency steering committee. This evaluation was also favourable and a copy of the report, along with an NCE management response can be found at: http://www.nce.gc.ca/pubs/reports/2007/evaluation/NCEEvaluationReport2007-eng.pdf.
B. Knowledge to Action
This program aims to build and strengthen teams of researchers and knowledge users engaged in KT at the community, regional, provincial or federal level. Applications received for this
initiative jumped from 30 in 2005 to 54 in 2007. Twelve of these 54 applications were funded in 2007-2008, representing an investment of approximately $2.2M over the next two years. Partners to date that
have supported this initiative include Canada Health Infoway and the Mental Health Commission of Canada.
C. Knowledge Synthesis
This program supports teams of researchers and health knowledge users to produce knowledge syntheses and scoping reviews that respond to the information needs of knowledge users in all areas of health.
When first launched in 2005, 16 applications were received with 8 projects funded. In 2007, 41 applications were received with 22 projects funded, representing nearly $2.0M in expenditures in fiscal year
2007-2008. CIHR also successfully negotiated a Tri-Council partnership focusing on syntheses on complex interactions between the environment and one or more other sectors - particularly
health, energy and natural resources, and information and communications technology. In addition CIHR forged partnerships with the Atlantic Advisory Committee on Health Human Resources,
the Canadian Patient Safety Institute, the Canadian Stroke Network, Health Canada,
the Mental Health Commission of Canada and the Western & Northern Health Human Resource Planning Forum.
D. The KT Award
Since 2003 CIHR has been raising awareness and celebrating KT excellence through the annual regional and national KT awards. These awards are granted
to an individual, team or organization that has made an outstanding contribution to increasing the application of research findings, improving the health of Canadians or strengthening the health system.
Each year CIHR gives out one national and one regional KT Award.
|
Benefits to Canadians - Reducing Injuries in the Workplace Manufacturing poor mental health? University invention reduces forces on people's backs |
Role of CIHR's 13 Institutes in Achieving KT
CIHR's Institutes play an instrumental role in helping to achieve CIHR's KT mandate as they are centrally located within the researcher, partner
and knowledge user communities. KT research is supported across the mandates of all 13 Institutes and in 2007-2008, 192 grants and awards totalling $9.5M were funded across the 13 institutes.
More than half of these grants and awards were funded through two institutes: the Institute of Health Services and Policy Research and the Institute of Population and Public Health. The KT
activities undertaken by the Institutes address their specific strategic priorities.
Program Activity 3.2: Support National Efforts to Capture the Economic Value for Canada of Health Research Advances made at Canadian Institutions
Commercialization is an integral part of CIHR's mandate and is part of the knowledge translation process. CIHR provides various funding programs in support of the implementation of its commercialization and innovation strategy, which focuses on four areas: research, talent, capital and linkages. More information on the strategy can be found at: http://www.cihr-irsc.gc.ca/e/30162.html.
Financial Resources ($M)
| Planned Spending | Authorities | Actual Spending |
|---|---|---|
| $27.3 | $103.4 | $98.3 |
Human Resources
| Planned | Actual | Difference |
|---|---|---|
| 13 | 12 | 1 |
|
Expected Results Implement strategies to enable the effective development and commercialization of health research that will lead to a better quality of life for Canadians through improvements in the Canadian health system, products and economy. As well, plan, launch and manage competitions and programs for grant funds to create and transfer new knowledge, strengthen Canadian capacity and networks and undertake effective commercialization of health research. |
Indicators
|
|
Link to Priority Priority #3: Knowledge Translation- Catalyze health innovation in order to strengthen health and the health-care system and contribute to the growth of Canada's economy. |
|
Program Activity 3.2 Performance Status: Exceeded Expectations
The following presents a 2007-2008 performance summary of the key sub-activities that support the performance status of Program Activity 3.2 - Support National Efforts to Capture the Economic Value for Canada of Health Research Advances made at Canadian Institutions.
As outlined in more detail in the sections below, CIHR has exceeded expectations in meeting the expected results for this program activity of implementing strategies to enable the effective development and commercialization of health research that will lead to a better quality of life for Canadians through improvements in the Canadian health system, products and economy. This performance rating is based primarily on an assessment of planned and actual spending, activities and outputs. Through an unplanned $163M increase from Budget 2007 CIHR was able to establish and launch the new Centres for Excellence for Commercialization and Research (CECR) program in collaboration with the other two granting councils SSHRC and NSERC. This innovative program has invested in research and commercialization centres capable of achieving global leadership in Canada. Other successes in CIHR's commercialization programs further support this rating as detailed below.
A. Centres of Excellence for Commercialization and Research (CECR)
The 2007 Federal Budget announced that as part of the S&T Strategy, approximately $163M in funding would be made available in 2007-2008 for the CECR Program, to be split among the three granting councils
- CIHR, NSERC and SSHRC. CIHR was granted $73.5M towards the CECR Program. Through the CECR
Program, the Federal Government is able to support research and commercialization centres capable of achieving global leadership for Canada and translating knowledge into significant commercial advantage.
The first CECR competition was launched in June of 2007. In 2007-2008 the Tri-councils committed the $163M in support of a total of eleven Centres of Excellence for Commercialization
and Research, 9 of which focus on health.
B. CIHR/Rx&D Collaborative Research Program
The CIHR/Rx&D Collaborative Research Program promotes peer-reviewed research and enhances the training and development of health research personnel and opportunities in Canada. This
was successfully completed in February 2007 with the launch of the Clinical Research Initiative (CRI) collaborative program with the
CFI. In 2007-2008, The CIHR/Rx&D Collaborative Research Program committed over $4.4M towards 199 new and ongoing grants and
awards. Private industry contributed over $6M16 in support of these same grants and awards. CIHR and its partner organizations have invested over $156M17 between 2000 and 2008 for research funded under this Program, over $45M of which was contributed by CIHR.
C. Proof of Principle (PoP)
CIHR identified a critical gap in funding at the early stage of commercialization, between the traditional role of granting agencies in supporting discovery research, and the demonstration
of "proof of principle" for an innovation, at which stage private-sector investment becomes interested. CIHR filled that gap with its PoP Program. To date, over 250 projects have been
funded and over $31M in CIHR commitments have been made through the PoP program. Over the first four years of competition funding, 76% of funded projects resulted in a new patent being
filed after receiving PoP funding (113 projects), 26% of funded PoP projects had intellectual property licenses (38 projects), and 14% of funded PoP projects contributed to new company formation (21 projects).
D. CIHR's Small and Medium-Size Enterprise (SME) Program
This program is designed for SMEs who are not members of Rx&D. The program supports a wide range of grants and awards, with fixed funding matches between CIHR's and
the company's contribution to the costs of a research grant or award. Eligible applicants may participate within and/or outside the Clinical Research Initiative. In 2007-2008 CIHR invested
a total of $4.5M in funding through the SME Program. This included funding for Fellowships, New Investigators, Research Chairs and Operating Grants. In addition, a total of $6M18 was contributed by SME partners in support of these applications over the same period.
16. Partner contributions are likely understated as the figures do not include "in-kind" partner contributions and some partner funds that are not administered by CIHR.
17. Partner contributions are likely understated as the figures do not include "in-kind" partner contributions and some partner funds that are not administered by CIHR.
18. Partner contributions are likely understated as the figures do not include "in-kind" partner contributions and some partner funds that are not administered by CIHR.
In 2007-08 CIHR provided approximately $13.7M in funding through its Commercialization programs focused on building successful commercialization activities within Canada's health research community (see Figure 13). CIHR contributed to creating the environment, the talent and the programs necessary for Canada to reap the economic benefits of health research: high-quality jobs; internationally-competitive biotechnology firms; increased direct foreign investment and increased productivity.
Figure 13: Commercialization Program Expenditures, 2000-2001 to 2007-2008
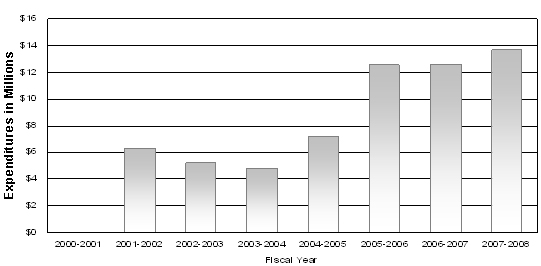
Source: CIHR Funding Database
|
Benefits to Canadians - Vulnerable Populations: Seniors Study links antipsychotics to dementia deaths Bilingual bonus: a delay in dementia Canadian Stroke Network
|
Risks and Challenges - Strategic Outcome 3.0
When delivering results in 2007-2008 related to Strategic Outcome 3.0 - Transforming Health Research into Action, CIHR proactively managed the following risks:
Risk # 1: Adequate Knowledge Translation: There is a risk that CIHR may not be able to support the creation and synthesis of knowledge and results to deliver on the knowledge translation portion of its mandate.
Impact: This could result in the inability to demonstrate impact, possible reductions in future funding levels and a lost opportunity to translate the results of the new knowledge created by CIHR funding into new products or medical services for the benefit of Canadians.
Mitigation: This risk is being mitigated in two ways. The first is the establishment of specific KT programs that require researchers to synthesize and disseminate their results. The second is the establishment of the infrastructure within CIHR to act as a convenor and to carry out the synthesis and dissemination of specific research results. CIHR is in the process of implementing a research reporting system which will allow the organization to access reports on the results of CIHR funded research. In addition, a "Knowledge to Action" strategy is being developed which outlines the roles of both CIHR and its partners in knowledge translation activities, including the appropriate translation of final grant reports.
Risk # 2: Effective reporting of results: There is a risk that CIHR may be unable to evaluate and report on the results of CIHR's funded-research inputs, outputs and impacts.
Impact: The linkages between health research inputs, outputs and impacts are difficult to trace when knowledge develops incrementally over time and through multiple channels. Attribution of credit for research impacts can also be complex, as impacts often result from a number of research projects carried out or funded either collaboratively or independently in the same and/or different countries. In addition, the application of research findings is influenced by a variety of contextual factors. This challenge could result in the inability to report on results, possible reductions in future funding levels and extensive public scrutiny.
Mitigation: To mitigate this risk CIHR has developed, and is in the process of implementing, an impact framework which provides guidance to CIHR and its partners on how to report on results in a consistent way to demonstrate impact.
Section III: Supplementary Information
Table 5: Departmental Link to Government of Canada Outcome Areas (for DPRs)
| Strategic Outcome: 1.0 Outstanding Research | ||||
| ($ millions) | Actual Spending 2007-2008 | Alignment to Government of Canada Outcome Area | ||
| Budgetary | Non-budgetary | Total | ||
| Activity 1.1 - Fund health research | $539.5 | $ - | $539.5 | Economic: An innovative and knowledge-based economy |
| Strategic Outcome: 2.0 Outstanding Researchers in Innovative Environments | ||||
| ($ millions) | Actual Spending 2007-2008 | Alignment to Government of Canada Outcome Area | ||
| Budgetary | Non-budgetary | Total | ||
| Activity 2.1 - Fund health researchers and trainees | $202.3 | $ - | $202.3 | Economic: An innovative and knowledge-based economy |
| Activity 2.2 - Fund research resources, collaboration and other grants to strengthen the health research community | $68.0 | $ - | $ 68.0 | Social: Healthy Canadians with access to quality health care |
| Activity 2.3 - Develop and support strong health research community through national and international alliances and priority setting | $24.0 | $ - | $24.0 | Social: Healthy Canadians with access to quality health care |
| Activity 2.4 - Inform research, clinical practice and public policy on ethical, social and legal issues (ELSI) related to health and health research | $2.2 | $ - | $2.2 | Social: Healthy Canadians with access to quality health care |
| Strategic Outcome: 3.0 Transforming Health Research into Action | ||||
| ($ millions) | Actual Spending 2007-2008 | Alignment to Government of Canada Outcome Area | ||
|
Budgetary |
Non-budgetary |
Total | ||
| Activity 3.1 - Support activities on knowledge translation, exchange, use and strategies to strengthen the health system | $39.8 | $ - | $39.8 | Social: Healthy Canadians with access to quality health care |
| Activity 3.2 - Support national efforts to capture the economic value for Canada of health research advances made at Canadian institutions | $98.3 | $ - | $98.3 | Economic: An innovative and knowledge-based economy |
Table 6: Comparison of Planned to Actual Spending (including FTEs)
| ($ millions) |
2005-2006 Actual |
2006-2007 Actual |
2007-2008 | |||
|
Main Estimates |
Planned Spending |
Total Authorities |
Actual |
|||
| Fund health research | 466.5 | 499.5 | 493.5 | 493.5 | 535.7 | 539.5 |
| Fund health researchers and trainees | 178.3 | 190.4 | 203.6 | 203.6 | 208.5 | 202.3 |
| Fund research resources, collaboration and other grants to strengthen the health research community | 70.0 | 66.2 | 70.0 | 70.0 | 69.7 | 68.0 |
| Develop and support a strong health research community through national and international alliances and priority setting | 23.4 | 23.3 | 28.1 | 28.1 | 28.2 | 24.0 |
| Inform research, clinical practice and public policy on ethical, legal and social issues (ELSI) related to health and health research | 1.9 | 2.2 | 6.3 | 6.3 | 6.3 | 2.2 |
| Support activities on knowledge translation, exchange, use and strategies to strengthen the health system | 35.4 | 35.0 | 40.7 | 40.7 | 41.9 | 39.8 |
| Support national efforts to capture the economic value for Canada of health research advances made at Canadian Institutions | 25.4 | 26.7 | 27.3 | 27.3 | 103.4 | 98.3 |
| Total | 800.9 | 843.3 | 869.5 | 869.5 | 993.7 | 974.1 |
| Less: Non‑respendable revenue | 4.1 | 2.4 | N/A | 2.8 | N/A | 3.1 |
| Plus: Cost of services received without charge | 4.8 | 5.2 | N/A | 5.5 | N/A | 5.6 |
| Total Departmental Spending | 801.6 | 846.1 | N/A | 872.2 | N/A | 976.6 |
| Full-time Equivalents | 324 | 347 | 406 | 406 | 406 | 361 |
Table 7: Voted and Statutory Items
|
Vote or Statutory Item |
Truncated Vote or Statutory Wording |
2007-2008 ($ millions) | |||
|
Main Estimates |
Planned Spending |
Total Authorities |
Actual | ||
| 15 | Operating expenditures | 42.5 | 42.5 | 45.1 | 42.8 |
| 20 | Grants and contributions | 822.4 | 822.4 | 944.0 | 926.7 |
| (S) | Contributions to employee benefit plans | 4.6 | 4.6 | 4.6 | 4.6 |
| Total | 869.5 | 869.5 | 993.7 | 974.1 | |
Table 8: Sources of Respendable and Non-Respendable Revenue
Non-Respendable Revenue
| ($ millions) |
Actual 2005-2006 |
Actual 2006-2007 |
2007-2008 | |||
|
Main Estimates |
Planned Revenue |
Total Authorities |
Actual | |||
| Fund health research | ||||||
| Refunds of Previous Years' Expenditures | 2.2 | 1.3 | N/A | 1.5 | N/A | 1.7 |
| Fund health researchers and trainees | ||||||
| Refunds of Previous Years' Expenditures | 1.1 | 0.6 | N/A | 0.8 | N/A | 0.8 |
| Fund research resources, collaboration and other grants to strengthen the health research community | ||||||
| Refunds of Previous Years' Expenditures | 0.3 | 0.2 | N/A | 0.2 | N/A | 0.2 |
| Develop and support a strong health research community through national and international alliances and priority setting | ||||||
| Refunds of Previous Years' Expenditures | 0.1 | 0.1 | N/A | 0.1 | N/A | 0.0 |
| Inform research, clinical practice and public policy on ethical, legal and social issues (ELSI) related to health and health research | ||||||
| Refunds of Previous Years' Expenditures | 0.1 | 0.0 | N/A | 0.0 | N/A | 0.1 |
| Support activities on knowledge translation, exchange, use and strategies to strengthen the health system | ||||||
| Refunds of Previous Years' Expenditures | 0.2 | 0.1 | N/A | 0.1 | N/A | 0.2 |
| Support national efforts to capture the economic value for Canada of health research advances made at Canadian Institutions | ||||||
| Refunds of Previous Years' Expenditures | 0.1 | 0.1 | N/A | 0.1 | N/A | 0.1 |
| Total Non-Respendable Revenue | 4.1 | 2.4 | N/A | 2.8 | N/A | 3.1 |
Table 9: Crosswalk - Performance Indicators Used in 2007-2008 RPP vs. 2007-2008 DPR
CIHR continues to make modifications to the set of performance indicators used to monitor its various program activities and sub-activities. In some cases the indicators used differ from those identified in the 2007-2008 RPP due to the availability of performance data or concerns that the data was not reliable. However, the indicators used in this report are consistent with those used in the DPR for 2006-2007.
| Program Activity and Expected Results | Performance Indicators Used in 2007-2008 RPP | Performance Indicators Used in 2007-2008 DPR |
|
1.1: Funding health research Effective and efficient funding programs that enable ethical health research creating health knowledge that responds to opportunities and priorities. |
1. Success of CIHR-funded research programs, including results, awareness and satisfaction levels 2. Extent to which Institutes have appropriately influenced the research, policy and/or practice agendas in their communities |
1. Level of activity: number and dollar value of investments 2. Success of CIHR-funded research programs, including results, awareness and satisfaction levels 3. Extent to which Institutes have appropriately influenced the research, policy and/or practice agendas in their communities |
|
2.1: Fund health researchers and trainees Effective and efficient funding programs that ensure a supply of highly trained health researchers and trainees are available to conduct outstanding research. |
1. Success of CIHR-funded salary and training programs, including results, awareness and satisfaction levels 2. Level and success of Institute activity in creating opportunities for capacity development based on successful initial and ongoing identification and targeting of research domains in need of capacity development |
1. Level of activity: number and dollar value of investments 2. Success of CIHR-funded salary and training programs, including results, awareness and satisfaction levels |
|
2.2: Fund research resources, collaboration and other grants to strengthen the health research community Effective and efficient partnerships and funding programs that lead to a dynamic research environment and outstanding research. |
1. Success of CIHR-funded research resources and collaboration programs, including results, awareness and satisfaction levels 2. Expenditure levels and distribution 3. Level of Institute leadership, activity and success in strengthening research infrastructure/environment |
1. Level of activity: number and dollar value of investments 2. Success of CIHR-funded research resources and collaboration programs, including results, awareness and satisfaction levels |
|
2.3: Develop and support a strong health research community through national and international alliances and priority-setting National and international research agendas are formulated and implemented. |
1. Success of CIHR-funded partnership research programs, including results, awareness and satisfaction levels 2. Number, diversity and scope of linkages, exchanges, alliances and partnerships with other organizations including health policy-makers at all levels of government (especially provincial governments) compared to baseline. Includes willingness of stakeholders to support research in Institute domains and number and size of funding flows through jointly-funded partnership programs where relevant |
1. Level of activity: number and dollar value of investments 2. Success of CIHR-funded partnership research programs, including results, awareness and satisfaction levels |
|
2.4: Inform research, clinical practice and public policy on ethical, legal and social issues (ELSI) related to health and health research. Uptake and application of ethics knowledge as an integral part of decision-making in health practice, research and policy. |
1. Success of CIHR's ELSI activities, for example, changes in the number of ethics-related incidents that arise from health practice, research, and policies 2. Number of publications resulting from ELSI research 3. Number of public policies influenced by ELSI principles 4. Opinions of health researchers, and policy-makers regarding their success in uptake and application of ethical knowledge |
1. Level of activity: number and dollar value of investments 2. Success of CIHR ELSI activities, including results, awareness and satisfaction levels |
| 3.1: Support activities on knowledge translation, exchange, use and strategies to strengthen the health system. Effective dissemination, exchange, synthesis and application of research results take place to create new knowledge, strengthen Canadian capacity and networks and, together with our partners, enable effective research and application of health research results. |
1. Success of CIHR-funded research programs, including results, awareness and satisfaction levels 2. Increased number, scope and diversity of knowledge translation activities supported by CIHR (and its partners where relevant) or resulting from CIHR activities (for example, synthesis papers, briefs, participation in policy task forces) compared to baseline 3. Identification of and initial communication with key knowledge translation stakeholders, followed by increased number of inputs (driven by research evidence) to stakeholders' decision processes |
1. Level of activity: number and dollar value of investments 2. Success of CIHR-funded research programs, including results, awareness and satisfaction levels |
| 3.2: Support national efforts to capture the economic value for Canada of health research advances made at Canadian institutions. Implement strategies to enable the effective development and commercialization of health research that will lead to a better quality of life for Canadians through improvements in the Canadian health system, products and economy. As well, plan, launch and manage competitions and programs for grant funds to create and transfer new knowledge, strengthen Canadian capacity and networks and undertake effective commercialization of health research. |
1. Success of CIHR-funded research programs, including results, awareness and satisfaction levels 2. Number and nature of patents, spin-off companies and licenses for intellectual property (IP) generated from CIHR-funded research |
1. Level of activity: number and dollar value of investments 2. Success of CIHR-funded research programs, including results, awareness and satisfaction levels. 3. Number and nature of patents, spin-off companies and licenses for intellectual property (IP) generated from CIHR-funded research. |
Table 10: Financial Statements
Canadian Institutes of Health Research
Management Responsibility for Financial Statements
Responsibility for the integrity and objectivity of the accompanying financial statements of the Canadian Institutes of Health Research (CIHR) for the year ended March 31, 2008 and all information contained in these statements rests with CIHR's management. These financial statements have been prepared by management in accordance with Treasury Board accounting policies and year-end instructions issued by the Office of the Comptroller General, which are consistent with Canadian generally accepted accounting principles for the public sector.
Management is responsible for the integrity and objectivity of the information in these financial statements. Some of the information in the financial statements is based on management's best estimates and judgement and gives due consideration to materiality. To fulfil its accounting and reporting responsibilities, management maintains a set of accounts that provides a centralized record of CIHR's financial transactions. Financial information submitted to the Public Accounts of Canada and included in CIHR's Departmental Performance Report and Annual Report is consistent with these financial statements.
Management maintains a system of financial management and internal control designed to provide reasonable assurance that financial information is reliable, that assets are safeguarded and that transactions are in accordance with the Financial Administration Act, are executed in accordance with prescribed regulations, within Parliamentary authorities, and are properly recorded to maintain accountability of Government funds and endowments. Management also seeks to ensure the objectivity and integrity of data in its financial statements by careful selection, training and development of qualified staff, by organizational arrangements that provide appropriate divisions of responsibility and by communications programs aimed at ensuring that regulations, policies, standards and managerial authorities are understood throughout the organization.
The Standing Committee on Performance Measurement, Evaluation and Audit, appointed by the Governing Council of CIHR, has reviewed these statements with management and the auditors, and has reported to the Governing Council. The Governing Council has approved the financial statements.
The financial statements of CIHR have been audited by the Auditor General of Canada, the independent auditor for the Government of Canada.
Approved by:
|
James Roberge, CMA Chief Financial Officer |
Pierre Chartrand, PhD Acting President |
May 30, 2008

Auditor's Report
To the Canadian Institutes of Health Research and the Minister of Health
I have audited the statement of financial position of the Canadian Institutes of Health Research (CIHR) as at March 31, 2008 and the statements of operations, equity and cash flow for the year then ended. These financial statements are the responsibility of CIHR's management. My responsibility is to express an opinion on these financial statements based on my audit.
I conducted my audit in accordance with Canadian generally accepted auditing standards. Those standards require that I plan and perform an audit to obtain reasonable assurance whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation.
In my opinion, these financial statements present fairly, in all material respects, the financial position of CIHR as at March 31, 2008 and the results of its operations and its cash flows for the year then ended in accordance with Canadian generally accepted accounting principles.
Nancy Y. Cheng, FCA
Assistant Auditor General
for the Auditor General of Canada
Ottawa, Canada
May 30, 2008
Canadian Institutes of Health Research
Statement of Operations
for the Year Ended March 31
(in thousands of dollars)
|
2008 |
2007 |
||
|
Expenses (Note 4) |
|||
| Health research | 547,858 | 511,042 | |
| Health researchers in innovative environments | 317,424 | 284,348 | |
| Transforming health research into action |
143,060 |
62,421 |
|
| Total Expenses |
1,008,342 |
857,811 |
|
|
Revenues (Note 5) |
|||
| Health research | 5,099 | 6,319 | |
| Health researchers in innovative environments | 2,954 | 3,516 | |
| Transforming health research into action |
1,332 |
772 |
|
| Total Revenues |
9,385 |
10,607 |
|
| Net Cost of Operations |
998,957 |
847,204 |
|
The accompanying notes are an integral part of these financial statements.
Canadian Institutes of Health Research
Statement of Financial Position
as at March 31
(in thousands of dollars)
| 2008 |
2007 |
|||
|---|---|---|---|---|
| Assets Financial Assets |
||||
|
Due from the Consolidated Revenue Fund |
36,371 | 15,751 | ||
| Accounts receivable: | ||||
| Other Federal Government departments | 296 | 678 | ||
| External parties | 465 | 395 | ||
| Advances |
196 |
196 |
||
|
Total financial assets |
37,328 | 17,020 | ||
| Non-financial assets | ||||
| Prepaid expenses | 82 | 445 | ||
| Tangible capital assets (Note 6) |
3,134 |
3,904 |
||
| Total non-financial assets |
3,216 |
4,349 |
||
|
Total Assets |
40,544 |
21,369 |
||
| Liabilities | ||||
| Accounts payable and accrued liabilities | ||||
| Other Federal Government departments | 465 | 444 | ||
| External parties | 3,894 | 2,577 | ||
| Gairdner Foundation grant (Note 7) | 20,000 | - | ||
| Vacation pay and compensatory leave | 1,316 | 1,110 | ||
| Deferred revenue (Note 8) | 12,011 | 12,730 | ||
| Employee severance benefits (Note 9) |
6,573 |
5,248 |
||
|
Total Liabilities |
44,259 |
22,109 |
||
|
Equity of Canada |
(3,715) |
(740) |
||
|
Total Liabilities and Equity of Canada |
40,544 |
21,369 |
||
Contingent liabilities (Note 10)
Contractual obligations (Note 11)
The accompanying notes are an integral part of these financial statements.
|
Approved by Governing Council: Pierre Chartrand, PhD |
Approved by Management: James Roberge, CMA |
Canadian Institutes of Health Research
Statement of Equity
as at March 31
(in thousands of dollars)
| 2008 |
2007 |
||
|---|---|---|---|
| Equity of Canada, Beginning of Year | (740) | (41) | |
| Net cost of operations | (998,957) | (847,204) | |
| Net cash provided by Government | 969,803 | 844,170 | |
| Change in Due from the Consolidated Revenue Fund | 20,620 | (2,889) | |
| Services provided without charge by other Government departments (Note 12) |
5,559 |
5,224 |
|
| Equity of Canada, End of Year |
(3,715) |
(740) |
|
The accompanying notes are an integral part of these financial statements.
Canadian Institutes of Health Research
Statement of Cash Flow
for the Year Ended March 31
(in thousands of dollars)
| 2008 |
2007 |
|||
|---|---|---|---|---|
| Operating Activities | ||||
| Net cost of operations | 998,957 | 847,204 | ||
| Non-cash items: | ||||
| Amortization of tangible capital assets | (1,868) | (1,498) | ||
| Services provided without charge by other Government departments | (5,559) | (5,224) | ||
| Gain on disposal of capital assets |
- |
4 |
||
| (7,427) | (6,718) | |||
| Variations in Statement of Financial Position: | ||||
| (Decrease) increase in accounts receivable and advances | (312) | 358 | ||
|
(Decrease) increase in prepaid expenses |
(363) | (97) | ||
|
(Increase) decrease in liabilities |
(22,150) |
2,074 |
||
|
(22,825) |
2,335 |
|||
| Cash Used by Operating Activities | 968,705 | 842,821 | ||
|
|
||||
| Capital Investment Activities | ||||
| Acquisitions of tangible capital assets | 1,098 | 1,358 | ||
|
Proceeds on disposal of capital assets |
- |
(9) |
||
| Cash Used by Capital Investment Activities |
1,098 |
1,349 |
||
| Financing Activities | ||||
| Net Cash Provided by Government of Canada |
969,803 |
844,170 |
||
The accompanying notes are an integral part of these financial statements.
Canadian Institutes of Health Research
Notes to the Financial Statements
for the Year Ended March 31, 2008
The Canadian Institutes of Health Research (CIHR) was established in June 2000 under the Canadian Institutes of Health Research Act, replacing the former Medical Research Council of Canada. It is listed in Schedule II to the Financial Administration Act as a departmental corporation.
CIHR's objective is to excel, according to international standards of scientific excellence, in the creation of new knowledge, and its translation into improved health, more effective health services and products, and a strengthened Canadian health care system. CIHR achieves these objectives through three strategic outcomes. The first strategic outcome is outstanding research, achieved by funding excellent and ethical health research across all disciplines that are relevant to health. The second strategic outcome is outstanding researchers in innovative environments, achieved by providing funding to develop and sustain health researchers in vibrant, innovative and stable research environments. The third strategic outcome is transforming health research into action, achieved by CIHR's knowledge translation activities and funding aimed to accelerate the transformation of research results into health benefits for Canadians and an improved health care system as well as helping to move new research breakthroughs toward potential commercial applications.
CIHR is led by a President who is the Chairperson of a Governing Council of not more than nineteen other members appointed by the Governor in Council. The Governing Council sets overall strategic direction, goals and policies and oversees programming, resource allocation, ethics, finances, planning and accountability.
CIHR has thirteen Institutes that focus on identifying the research needs and priorities for specific health areas, or for specific populations, then developing strategic initiatives to address those needs. Each Institute is led by a Scientific Director who is guided by an Institute Advisory Board, which strives to include representation of the public, researcher communities, research funders, health professionals, health policy specialists and other users of research results.
CIHR's grants, awards, and operating expenditures are funded by budgetary authorities. Employee benefits are funded by statutory authorities.
2. Significant Accounting Policies
These financial statements have been prepared in accordance with Treasury Board accounting policies and year-end instructions issued by the Office of the Comptroller General, which are consistent with Canadian generally accepted accounting principles for the public sector. The most significant accounting policies are as follows:
(a) Parliamentary appropriations - CIHR is financed by the Government of Canada through Parliamentary appropriations. Appropriations provided to CIHR do not parallel financial reporting according to generally accepted accounting principles since appropriations are primarily based on cash flow requirements. Consequently, items recognized in the statement of operations and the statement of financial position are not necessarily the same as those provided through appropriations from Parliament. Note 3 provides a high-level reconciliation between the bases of reporting.
(b) Net cash provided by government - CIHR operates within the Consolidated Revenue Fund (CRF), which is administered by the Receiver General for Canada. All cash received by CIHR is deposited to the CRF and all cash disbursements made by CIHR are paid from the CRF. The net cash provided by Government is the difference between all cash receipts and all cash disbursements including transactions between departments of the Federal Government.
(c) Due from the Consolidated Revenue Fund represents the amount of cash that CIHR is entitled to draw from the Consolidated Revenue Fund without further appropriations, in order to discharge its liabilities.
(d) Revenues
- Funds received from external parties for specified purposes are recorded upon receipt as deferred revenues. These revenues are recognized in the period in which the related expenses are incurred.
- Other revenues are accounted for in the period in which the underlying transaction or event occurred that gave rise to the revenues.
(e) Expenses - Expenses are recorded on the accrual basis:
- Grants and awards are recognized when the entitlement has been established, the recipient has met the eligibility criteria, and program authority exists.
- Vacation pay and compensatory leave are expensed as the benefits accrue to employees under their respective terms of employment.
- Services provided without charge by other government departments are recorded as operating expenses at their estimated cost.
(f) Refunds of previous years' expenses - These amounts include the return of grants and awards funds to CIHR in the current fiscal year for expenses incurred in previous fiscal years due to cancellations; refunds of previous years' expenses related to goods or services; and adjustments of previous years' accounts payable. These refunds and adjustments are recorded as expenses in the financial statements but are recorded as revenue on an appropriation basis and therefore are excluded when determining current year appropriations used.
(g) Employee future benefits
Pension benefits: Eligible employees participate in the Public Service Pension Plan, a multiemployer defined benefit plan administered by the Government of Canada. CIHR's contributions to the Plan are charged to expenses in the year incurred and represent the total obligation of CIHR to the Plan. Current legislation does not require CIHR to make contributions for any actuarial deficiencies of the Plan.
Severance benefits: Employees are entitled to severance benefits under labour contracts or conditions of employment. These benefits are accrued as employees render the services necessary to earn them. The obligation relating to the benefits earned by employees is calculated using information derived from the results of the actuarially determined liability for employee severance benefits for the Government as a whole.
(h) Accounts receivable - These are stated at amounts expected to be ultimately realized.
A provision for doubtful accounts is made for any amounts where recovery is considered uncertain.
(i) Contingent liabilities - Contingent liabilities are potential liabilities which may become actual liabilities when one or more future events occur or fail to occur. To the extent that the future event is likely to occur or fail to occur, and a reasonable estimate of the loss can be made, an estimated liability is accrued and an expense is recorded. If the likelihood is not determinable or an amount cannot be reasonably estimated, the contingency is disclosed in the notes to the financial statements.
(j) Tangible capital assets - All tangible capital assets having an individual initial cost of $5,000 or more are recorded at their acquisition cost. Amortization of tangible capital assets is done on a straight-line basis over the estimated useful life of the capital asset as follows:
| Asset Class | Amortization Period |
|---|---|
| Informatics hardware | 3-5 years |
| Informatics software | 3 years |
| Office equipment | 10 years |
| Motor vehicles | 5 years |
Amounts included in work-in-progress are uncompleted capital projects which are transferred to the appropriate asset class upon completion, and are then amortized according to CIHR's policy.
(k) Measurement uncertainty - The preparation of these financial statements in accordance with Treasury Board accounting policies and year-end instructions issued by the Office of the Comptroller General, which are consistent with Canadian generally accepted accounting principles for the public sector, requires management to make estimates and assumptions that affect the amounts of assets, liabilities, revenues and expenses reported in the financial statements. At the time of preparation of these statements, management believes the estimates and assumptions to be reasonable. The most significant items where estimates are used are contingent liabilities, the liability for vacation pay and compensatory leave, employee severance benefits, the useful life of tangible capital assets, and services provided without charge. Actual results could differ significantly from those estimated. Management's estimates are reviewed periodically and, as adjustments become necessary, they are recorded in the financial statements in the year they become known.
3. Parliamentary Appropriations
CIHR receives most of its funding through annual parliamentary appropriations. Items recognized in the statement of operations and the statement of financial position in one year may be funded through parliamentary appropriations in prior, current or future years. Accordingly, CIHR has different net results of operations for the year on a government funding basis than on an accrual accounting basis. The differences are reconciled in the following tables:
(a) Reconciliation of net cost of operations to current year appropriations used
(in thousands of dollars)
| 2008 |
2007 |
|||
|---|---|---|---|---|
| Net cost of operations | 998,957 | 847,204 | ||
|
Adjustments for items affecting net cost of operations but not affecting appropriations: |
||||
| Add (Less): | ||||
| Services provided without charge | (5,559) | (5,224) | ||
| Gairdner Foundation grant (Note 7) | (20,000) | - | ||
| Gain on disposal of capital assets | - | 4 | ||
| Refunds of previous years' expenses | 3,087 | 2,432 | ||
| Employee severance benefits | (1,325) | (615) | ||
| Amortization of tangible capital assets | (1,868) | (1,498) | ||
| Vacation pay and compensatory leave | (206) | (200) | ||
| Other adjustments |
249 |
(94) |
||
| (25,622) | (5,195) | |||
|
Adjustments for items not affecting net cost of operations but affecting appropriations |
||||
| Add (Less): | ||||
| Acquisitions of tangible capital assets | 1,098 | 1,358 | ||
| Prepaid expenses |
(363) |
(97) |
||
| Current year appropriations used |
974,070 |
843,270 |
||
(b) Appropriations provided and used
(in thousands of dollars)
| 2008 |
2007 |
|
|---|---|---|
| Parliamentary appropriations provided: | ||
| Vote 15 - Operating expenditures | 45,060 | 43,021 |
| Less: | ||
| Lapsed appropriation |
(2,333) |
(3,657) |
|
42,727 |
39,364 |
|
| Vote 20 - Grants | 943,967 | 816,183 |
| Less: | ||
| Lapsed appropriation |
(17,251) |
(16,536) |
| 926,716 | 799,647 | |
| Statutory contributions to employee benefit plans |
4,627 |
4,259 |
| Current year appropriations used |
974,070 |
843,270 |
(c) Reconciliation of net cash provided by Government to Parliamentary appropriations used
(in thousands of dollars)
| 2008 |
2007 |
||
|---|---|---|---|
| Net cash provided by Government | 969,803 | 844,170 | |
| Refunds of previous years' expenses | 3,087 | 2,432 | |
| Cash proceeds on disposal of capital assets |
- |
9 |
|
|
972,890 |
846,611 |
||
| Change in net position in the Consolidated Revenue Fund | |||
| Variation in accounts receivable and advances | 312 | (358) | |
| Variation in accounts payable and accrued liabilities | 1,338 | (1,273) | |
| Variation in deferred revenue | (719) | (1,616) | |
| Other adjustments |
249 |
(94) |
|
|
|
1,180 |
(3,341) |
|
| Current year appropriations used |
974,070 |
843,270 |
|
4. Expenses
(in thousands of dollars)
| 2008 |
2007 |
||
|---|---|---|---|
| Grants and awards | |||
| Open competitions | 516,541 | 487,917 | |
| Strategic initiatives | 210,842 | 195,762 | |
| Gairdner Foundation grant (Note 7) | 20,000 | - | |
| Institute support grants | 13,000 | 13,000 | |
| Knowledge translation | 8,224 | 3,864 | |
| Canada Research Chairs | 86,482 | 82,205 | |
| Networks of Centres of Excellence | 27,500 | 27,500 | |
| Centres of Excellence in Commercialization and Research |
73,512 |
- |
|
| Total grants and awards | 956,101 | 810,248 | |
| Less: Refunds of previous years' grants and awards |
(3,087) |
(1,972) |
|
|
953,014 |
808,276 |
||
| Operations and administration | |||
| Salaries and employee benefits | 36,551 | 31,683 | |
| Professional and special services | 5,300 | 4,845 | |
| Travel | 3,696 | 3,425 | |
| Accommodation | 3,399 | 3,314 | |
| Amortization of tangible capital assets | 1,868 | 1,498 | |
| Furniture, equipment and software | 1,813 | 1,998 | |
| Communication | 1,439 | 1,450 | |
| Other |
1,262 |
1,322 |
|
| Total operations and administration |
55,328 |
49,535 |
|
| Total Expenses |
1,008,342 |
857,811 |
|
5. Revenues
(in thousands of dollars)
The following are the revenues recognized for the year:
| 2008 |
2007 |
|
|---|---|---|
| Donations for health research | 9,235 | 9,362 |
| Cost sharing agreements with other Government departments | 150 | 1,240 |
| Gain on disposal of capital assets | - | 4 |
| Endowments for health research |
- |
1 |
| Total Revenues |
9,385 |
10,607 |
6. Tangible Capital Assets
(in thousands of dollars)
| Cost | Accumulated amortization | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Capital asset class | Opening balance | Acquisitions |
Transfers, disposals and write-offs |
Closing balance | Opening balance | Amortization |
Transfers, disposals and write-offs |
Closing balance |
2008 Net Book Value |
2007 Net Book Value |
| Informatics hardware | 1,928 | 142 | - | 2,070 | 1,546 | 169 | - | 1,715 | 355 | 382 |
| Informatics software | 7,780 | 953 | - | 8,733 | 4,531 | 1,659 | - | 6,190 | 2,543 | 3,249 |
| Office equipment | 345 | - | - |
345 |
123 |
35 |
- | 158 | 187 | 222 |
| Vehicles | 32 | - | - |
32 |
4 | 5 | - | 9 | 23 | 28 |
| Work-in-progress | 23 | 3 | - | 26 | - | - | - | - | 26 | 23 |
| Total | 10,108 | 1,098 | - | 11,206 | 6,204 | 1,868 | - |
8,072 |
3,134 | 3,904 |
Amortization expense (in thousands of dollars) for the year ended March 31, 2008 is $1,868 (2007 - $1,498).
On March 31, 2008, CIHR entered into a funding agreement with the Gairdner Foundation, a not-for-profit, independent organization devoted to the recognition of outstanding achievement in health research worldwide. CIHR agreed to provide the Gairdner Foundation with a grant at the requisition of the Minister of Health in the amount of $20,000,000. The purpose of the endowment is to support and enhance the Gairdner International Awards, which are among the world's most respected health prizes. The Gairdner Foundation has proposed to use the investment proceeds from the endowment to increase the value of each Gairdner International Award to $100,000 in keeping with their stature. The endowment will also be used to establish a new individual award for global health to be named the "Canada Gairdner Global Health Award". After the endowment is disbursed, the Gairdner International Awards will be renamed the "Canada Gairdner International Awards".
Monies received as donations from various organizations and individuals for health research as well as interest on endowments are recorded as deferred revenue until such time as they are disbursed in accordance with agreements between the contributor and CIHR or in accordance with the terms of the endowments.
The transactions relating to these accounts are as follows:
(in thousands of dollars)
| 2008 |
2007 |
|||
|---|---|---|---|---|
| Donations for health research | ||||
| Balance, beginning of the year | 12,726 | 14,344 | ||
| Add: | ||||
| Donations received | 8,049 | 7,191 | ||
| Interest earned | 465 | 553 | ||
| Less: | ||||
| Grants expensed |
9,235 |
9,362 |
||
| Balance, end of the year |
12,005 |
12,726 |
||
| Interest on endowments for health research | ||||
| Balance, beginning of the year | 4 | 2 | ||
| Add: | ||||
| Interest earned | 3 | 3 | ||
| Less: | ||||
| Miscellaneous expenses |
1 |
1 |
||
| Balance, end of the year |
6 |
4 |
||
| Total deferred revenue |
12,011 |
12,730 |
||
Employees of CIHR are entitled to specific benefits on or after termination or retirement, as provided for under various collective agreements or conditions of employment.
(a) Pension benefits: CIHR's employees participate in the Public Service Pension Plan, which is sponsored and administered by the Government of Canada. Pension benefits accrue up to a maximum period of 35 years at a rate of 2% per year of pensionable service, multiplied by the average of the best five consecutive years of earnings. The benefits are integrated with the Canada/Quebec Pension Plans benefits and they are indexed to inflation. Both the employees and CIHR contribute to the cost of the Plan. CIHR's responsibility with regard to the Plan is limited to its contributions. Actuarial surpluses or deficiencies are recognized in the financial statements of the Government of Canada, as the Plan's sponsor.
The 2007-08 expense represents approximately 2.1 times (2.3 in 2006-07) the contributions by employees.
CIHR's and employees' contributions to the Public Service Pension Plan for the year were as follows:
(in thousands of dollars)
| 2008 |
2007 |
|
|---|---|---|
| CIHR's contributions | 3,373 | 3,139 |
| Employees' contributions | 1,584 | 1,378 |
(b) Severance benefits: CIHR provides severance benefits to its employees based on eligibility, years of service and
final salary. These severance benefits are not pre-funded. Benefits will be paid from future appropriations. Information about the severance benefits, measured as at March 31, is as follows:
(in thousands of dollars)
| 2008 |
2007 |
|
|---|---|---|
| Accrued benefit obligation, beginning of year |
5,248 |
4,633 |
| Expense for the year | 1,624 | 898 |
| Benefits paid during the year |
(299) |
(283) |
| Accrued benefit obligation, end of year |
6,573 |
5,248 |
A legal suit for employment equity was initiated by the Public Service Alliance of Canada against Her Majesty the Queen naming certain separate employer organizations of the Government of Canada, including the Canadian Institutes of Health Research (CIHR), as defendants. The amount of this claim, as it relates to CIHR, is estimated to be $747,000. In management's opinion, the outcome of this litigation is not presently determinable and no estimated liability has been accrued or expense recorded in the financial statements. CIHR may be subject to other claims in the normal course of business. In management's view, these claims do not have any material impact on the financial statements and consequently, no provision has been made for these claims.
CIHR is committed to disburse grants and awards in future years subject to the appropriation of funds by Parliament. In addition, the nature of CIHR's operating activities result in some multi-year contracts whereby CIHR will be committed to make some future payments when the goods or services are rendered. Future year contractual obligations are as follows:
| (in thousands of dollars) | 2009 | 2010 | 2011 | 2012 | 2013 and thereafter | Total |
|---|---|---|---|---|---|---|
| Grants and awards | 739,175 | 537,309 | 363,679 | 197,477 | 119,781 | 1,957,421 |
|
Operating |
2,091 | 418 | 2 | - | - | 2,511 |
| Total | 741,266 | 537,727 | 363,681 | 197,477 | 119,781 | 1,959,932 |
12. Related Party Transactions
CIHR is related in terms of common ownership to all Government of Canada departments, agencies, and Crown Corporations. CIHR enters into transactions with these entities in the normal course of business and on normal trade terms.
(a) Services provided without charge by other Government departments
During the year, CIHR received services which were obtained without charge from other Government departments. The estimated costs of these services have been included as an expense
in the department's Statement of Operations in the following amounts:
(in thousands of dollars)
| 2008 |
2007 |
|
|---|---|---|
|
Accommodation provided by Public Works and Government Services Canada |
3,399 | 3,314 |
|
Employer's contribution to the health and dental insurance plans provided by Treasury Board Secretariat |
2,027 | 1,772 |
|
Audit services provided by the Office of the Auditor General of Canada |
133 |
138 |
|
Total services provided without charge by other Government departments |
5,559 |
5,224 |
(b) Administration of programs on behalf of other Government departments
CIHR administers funds received from other federal departments and agencies to issue grants, awards and related payments on their behalf. During the year, CIHR administered $150,000 ($1,239,838 in 2007) in funds for grants and awards. These amounts are reflected in CIHR's Statement of Operations as both revenues and expenses.
(c) Administration of CIHR funds by other Government departments
Other federal departments and agencies administer funds on behalf of CIHR to issue grants, awards and related payments. During the year, other federal departments and agencies administered $91,061,335 ($87,331,623 in 2007) in funds for grants and awards, primarily pertaining to the Canada Research Chairs program. These amounts are reflected in CIHR's Statement of Operations as expenses.
The fair values of financial assets and liabilities approximate the carrying amounts of these instruments due to the short period to maturity.
Table 11: Details on Transfer Payment Programs (TPPs)
| Name of Transfer Payment Program: Grants for research projects and personnel support | ||||||
| Start Date: October 2000 | End Date: N/A | |||||
| Description: CIHR administers a large suite of grant programs all of which are listed in its Grants and Awards Guide and/or made available publicly on the web http://www.cihr.gc.ca/. For each program, the website provides a description of the program, eligibility criteria, application guidelines and forms, and policies and procedures governing the use of funds. | ||||||
| Strategic Outcomes: 1.0 - Fund Health Research, 2.0 - Fund Health Researchers and Trainees, 3.0 - Support Activities on Knowledge Translation, Exchange and Use | ||||||
| Results Achieved: Please refer to section II of this DPR (Analysis by Strategic Outcome) for detailed information on the achieved results. | ||||||
| ($ millions) |
Actual Spending 2005-2006 |
Actual Spending 2006-2007 | Planned Spending 2007-2008 | Total Authorities 2007-2008 |
Actual Spending 2007-2008 |
Variance(s) [Actual / Planned] |
| Program Activity 1.1 - Fund Health Research | ||||||
| Total Grants | $ 443.9 | $ 476.4 | $ 468.7 | $ 509.5 | $ 514.4 | ($ 45.7) |
| Total Contributions | - | - | - | - | - | - |
| Total Other Types of TPs | - | - | - | - | - | - |
| Total Program Activity | $ 443.9 | $ 476.4 | $ 468.7 | $ 509.5 | $ 514.4 | ($ 45.7) |
| Program Activity 2.1 - Fund Health Researchers | ||||||
| Total Grants | $ 158.5 | $ 168.6 | $ 185.0 | $ 185.3 | $ 175.6 | $ 9.4 |
| Total Contributions | - | - | - | - | - | - |
| Total Other Types of TPs | - | - | - | - | - | - |
| Total Program Activity | $ 158.5 | $ 168.6 | $ 185.0 | $ 185.3 | $ 175.6 | $ 9.4 |
| Program Activity 2.2 - Fund Research Resources, Collaboration and Other Grants to Strengthen the Health Research Community | ||||||
| Total Grants | $ 66.6 | $ 62.7 | $ 67.3 | $ 66.9 | $ 64.2 | $ 3.1 |
| Total Contributions | - | - | - | - | - | - |
| Total Other Types of TPs | - | - | - | - | - | - |
| Total Program Activity | $ 66.6 | $ 62.7 | $ 67.3 | $ 66.9 | $64.2 | $ 3.1 |
| Program Activity 2.3 - Develop and Support Strong Health Research Community through National and International Alliances and Priority-Setting | ||||||
| Total Grants | $ 9.1 | $ 9.0 | $ 10.8 | $ 10.8 | $ 9.5 | $ 1.3 |
| Total Contributions | - | - | - | - | - | - |
| Total Other Types of TPs | - | - | - | - | - | - |
| Total Program Activity | $ 9.1 | $ 9.0 | $ 10.8 | $ 10.8 | $ 9.5 | $ 1.3 |
| Program Activity 2.4 - Inform Research, Clinical Practice and Public Policy on Ethical, Legal and Social Issues (ELSI) Related to Health and Health Research | ||||||
| Total Grants | $ 1.4 | $ 1.7 | $ 3.8 | $ 3.8 | $ 1.8 | $ 2.0 |
| Total Contributions | - | - | - | - | - | - |
| Total Other Types of TPs | - | - | - | - | - | - |
| Total Program Activity | $ 1.4 | $ 1.7 | $ 3.8 | $ 3.8 | $ 1.8 | $ 2.0 |
| Program Activity 3.1 - Support Activities on Knowledge Translation, Exchange, Use and Strategies to Strengthen the Health System | ||||||
| Total Grants | $ 33.3 | $ 32.8 | $ 37.7 | $ 38.7 | $ 37.4 | $ 0.3 |
| Total Contributions | - | - | - | - | - | - |
| Total Other Types of TPs | - | - | - | - | - | - |
| Total Program Activity | $ 33.3 | $ 32.8 | $ 37.7 | $ 38.7 | $ 37.4 | $ 0.3 |
| Program Activity 3.2 - Support National Efforts to Capture the Economic Value for Canada of Health Research | ||||||
| Total Grants | $ 24.2 | $ 25.4 | $ 25.6 | $ 28.1 | $ 23.4 | $ 2.2 |
| Total Contributions | - | - | - | - | - | - |
| Total Other Types of TPs | - | - | - | - | - | - |
| Total Program Activity | $ 24.2 | $ 25.4 | $ 25.6 | $ 28.1 | $ 23.4 | $ 2.2 |
| Comment(s) on Variance(s): The lapsed funding in the Grants and Awards was the result of difficulties experienced by universities in filling Canada Research Chairs at the rate that had been hoped for. | ||||||
|
Activities completed in 2007-2008: Results Based Management Accountability Frameworks (RMAF) Completed:
Evaluation Reports Completed and Approved in 2007-2008: STIHR Evaluation: Key stakeholders considered the STIHR to be comparable with programs like the Canada Graduate Scholarships, the Doctoral Research Awards, and CIHR Fellowship awards in terms of trainees' disciplinary background; early scholarly productivity; and perceptions of the training environment and trainee experience. Integrated Report of the Evaluation of CIHR's 13 Institutes: Relevance: To what extent is there still a need for this Institute to support the development of Canadian capacity and research excellence in this field of health research? CIHR as a whole and each of the 13 Institutes remain a relevant and needed component of support to health research in Canada. Their mandates and strategic priorities are regarded as appropriate and relevant. However, views were expressed for most Institutes that their mandates are very broad given their available resources. Delivery: What has been the influence of other factors on the overall effectiveness of Institutes? All 13 Institutes have been successful in establishing effective organizations and program delivery. The evaluation results showed that all 13 Institutes have used strategic and operational planning mechanisms effectively, and that the consultative processes used in these mechanisms have strengthened linkages and engagement of stakeholder communities. Effectiveness: How effectively has this Institute achieved its objectives, fulfilled its mandate and mission, and achieved its vision? How effectively and uniquely has this Institute contributed to the overall objective of the CIHR? Overall, the evaluations showed that the Institutes have performed well, making substantial progress in fulfilling their mandates and strategic priorities. The greatest effectiveness was noted in the areas of creating new knowledge, developing health research capacity, and developing partnerships and collaborations through a broad range of innovative initiatives. Although a priority, knowledge translation has been a significant challenge for the majority of Institutes. Institute evaluations suggested that they have struggled with a lack of clarity on the vision and definition of knowledge translation within CIHR. Alternatives: Are there alternative ways to achieve the same or better results in terms of research capacity, excellence and impacts in this research domain with greater efficiency? While the issue was explored through the evaluations, the determination was that no-viable alternative to the Institute model was presented. Networks of Centers of Excellence (NCE) (Tri-Agency - NSERC
lead agency): Performance Measurement Studies: Evaluability Assessment: Other Substantive Studies/Reviews:
Activities planned for in 2008-2009: A Corporate 5-Year Evaluation Plan is being finalized based upon a risk-based 5-year evaluation prioritization exercise and approved schedule. The work for 2008-2009 includes: (1) completion of the Tri-agency Canada Graduate Scholarship evaluation; (2) completion of the Doctoral Research Award Evaluation; (3) completion of STIHR case (4) initiation of an evaluation of Team-Type Programs (5) initiation of studies as part of an Operating Grant Program evaluation (6) initiation of an evaluation study of Randomized Controlled Trials program (7) participation in Tri-Council evaluations of the Indirect Costs Program and of the Tri-Council Panel and Secretariat on Research Ethics |
||||||
|
The approved Risk-Based Annual Internal Audit Plan for 2008-2009 includes audits of (1) the Non-Financial Administration of Open Operating Grants and (2) the Financial Administration of Open Operating Grants. These audits are expected to be completed by December 31, 2008. In addition, the approved Risk Assessment and Risk-Based 5-Year Internal Audit Plan includes audits of the Non-Financial Administration of (1) the Salary Program - in 2009-2010 (2) Training Program - in 2010-2011 and (3) Research Related Activity - in 2011-2012. The timing and scope of these future audits may change as a result of the 2008-2009 audits of Open Operating Grants, the results of audits by the Office of the Auditor General and the Office of the Comptroller General, and TBS priorities. |
||||||
| Name of Transfer Payment Program: Institute Support Grants (ISG) | ||||||
| Start Date: October 2000 | 3) End Date: N/A | |||||
| Description: Health Research Institutes will assess research priorities in their area, determine gaps and opportunities that present research is not addressing, and will devote resources toward answering these questions and addressing these gaps. Payment of Institute Support Grants will be integrated into CIHR's payment systems currently in place for Research Funding Programs. These Programs are paid in bi-monthly installments and are in compliance with TBS's policy on transfer payments. | ||||||
| Strategic Outcomes: 2.0 - Fund Health Researchers and Trainees | ||||||
| Results Achieved: Please refer to section II of this DPR (Analysis by Strategic Outcome) for detailed information on the achieved results. | ||||||
| ($ millions) |
Actual Spending 2005-2006 |
Actual Spending 2006-2007 | Planned Spending 2007-2008 | Total Authorities 2007-2008 |
Actual Spending 2007-2008 |
Variance(s) [Actual / Planned] |
| Program Activity 2.3 - Develop and Support Strong Health Research Community through National and International Alliances and Priority-Setting | ||||||
| Total Grants | $ 13.0 | $ 13.0 | $ 13.0 | $ 13.0 | $ 13.0 | - |
| Total Contributions | - | - | - | - | - | - |
| Total Other Types of TPs | - | - | - | - | - | - |
| Total Program Activity | $ 13.0 | $ 13.0 | $ 13.0 | $ 13.0 | $ 13.0 | - |
| Comment(s) on Variance(s): N/A | ||||||
| The approved Risk Assessment and Risk-Based 5-Year Internal Audit Plan does not include an audit of ISGs. | ||||||
| Name of Transfer Payment Program: Canada Graduate Scholarships | ||||||
| Start Date: Fiscal Year 2003-2004 | End Date: N/A | |||||
| Description: The Canada Graduate Scholarships Program administered by CIHR is intended to provide special recognition and support to students who are pursuing a Master's or Doctoral degree in a health related field in Canada. These candidates are expected to have an exceptionally high potential for future research achievement and productivity. This program awards scholarships through national competitions by the granting agencies; NSERC, SSHRC, and CIHR. These awards are intended to sustain recipients while they pursue graduate studies. | ||||||
| Strategic Outcomes: 2.0 - Fund Health Researchers and Trainees | ||||||
| Results Achieved: Please refer to section II of this DPR (Analysis by Strategic Outcome) for detailed information on the achieved results. | ||||||
| ($ millions) |
Actual Spending 2005-2006 |
Actual Spending 2006-2007 | Planned Spending 2007-2008 | Total Authorities 2007-2008 |
Actual Spending 2007-2008 |
Variance(s) [Actual / Planned] |
| Program Activity 2.1 - Fund Health Researchers and Trainees | ||||||
| Total Grants | $ 8.1 | $ 10.1 | $ 10.5 | $ 14.4 | $ 13.9 | ($ 3.4) |
| Total Contributions | - | - | - | - | - | - |
| Total Other Types of TPs | - | - | - | - | - | - |
| Total Program Activity | $ 8.1 | $ 10.1 | $ 10.5 | $ 14.4 | $ 13.9 | ($ 3.4) |
| Comment(s) on Variance(s): N/A | ||||||
| A "Tri-Agency" evaluation of the CGS program, led by CIHR, was initiated in Fall 2007-2008 and is expected to be completed in late 2008-2009. | ||||||
| The approved Risk Assessment and Risk-Based 5-Year Internal Audit Plan does not include an audit of CGS. | ||||||
| Name of Transfer Payment Program: Centres of Excellence for Commercialization and Research | ||||||
| Start Date: Fiscal Year 2007-2008 | End Date: 2011-12 | |||||
| Description: The Centres of Excellence for Commercialization and Research (CECR) Program supports research and commercialization centres capable of achieving global leadership for Canada and translating knowledge into significant commercial advantage. CECR is a joint program of the Tri-council, in partnership with Industry Canada. Through this program, the Federal Government will identify the best initiatives based on international peer review and advice from a Private Sector Advisory Board, and make investments in partnership with others, such as the provinces and businesses. | ||||||
| Strategic Outcomes: 3.0 - Support Activities on Knowledge Translation, Exchange and Use | ||||||
| Results Achieved: Please refer to section II of this DPR (Analysis by Strategic Outcome) for detailed information on the achieved results. | ||||||
| ($ millions) |
Actual Spending 2005-2006 |
Actual Spending 2006-2007 | Planned Spending 2007-2008 | Total Authorities 2007-2008 |
Actual Spending 2007-2008 |
Variance(s) [Actual / Planned] |
| Program Activity 2.1 - Fund Health Researchers and Trainees | ||||||
| Total Grants | - | - | - | $ 73.5 | $ 73.5 | ($ 73.5) |
| Total Contributions | - | - | - | - | - | - |
| Total Other Types of TPs | - | - | - | - | - | - |
| Total Program Activity | - | - | - | $ 73.5 | $ 73.5 | ($ 73.5) |
| Comment(s) on Variance(s): N/A | ||||||
| A "Tri-Agency evaluation was recently completed of the Networks of Centres of Excellence which subsumes the Centres of Excellence for Commercialization and Research as part of its portfolio. The Centres of Excellence for Commercialization and Research is a new program that was launched in Summer of 2007-2008, therefore no evaluation was completed for this program in 2007-2008. | ||||||
| The approved Risk Assessment and Risk-Based 5-Year Internal Audit Plan does not include an audit of CECR. | ||||||
Table 12: Internal Audits and Evaluations
The following table identifies a list of planned evaluations and audits at CIHR for 2007-2008.
| Planned Internal Audit or Evaluation | Estimated Start Date | Estimated Completion Date |
|---|---|---|
| Audit of the Electronic Information System (EIS) | April 2007 | Completed: October 2007 |
| Audit of the Acquisition Cards Program | June 2007 | Completed: November 2007 |
| Audit of Delegation of Financial Signing Authorities | September 2007 | Completed: February 2008 |
| Audit of the Report on Plans and Priorities (RPP) | September 2007 | Completed: February 2008 |
| Audit of Research Ethics | Carried forward from 2007-08 to 2008-09 | March 2009 |
| Evaluation of the Strategic Training Initiative in Health Research | In progress | Actual completion date: June 2008 |
| Evaluation of the Canada Graduate Scholarships Program (4th-year review) | In progress | Estimated completion date: October 2008 |
| Summative Evaluation of the Interdisciplinary Health Research Teams and Community Alliances in Health Research Programs | This project has been cancelled | This evaluation has been integrated with the evaluation of CIHR team type programs. The framework for the team type programs evaluation was completed in April 2008. |
| Evaluation of the Small Health Organization Partnership Program | October 2007 | |
| Evaluation Framework for the Operating Grants Program | In progress | Estimated completion date: October 2008 |
| Evaluation Framework for the CIHR/Rx&D Program | N/A | This project has been cancelled due to a lack of financial resources. |
| Evaluation Framework for Obesity and Healthy Body Weights Program | In progress | Actual completion date: June 2008 |